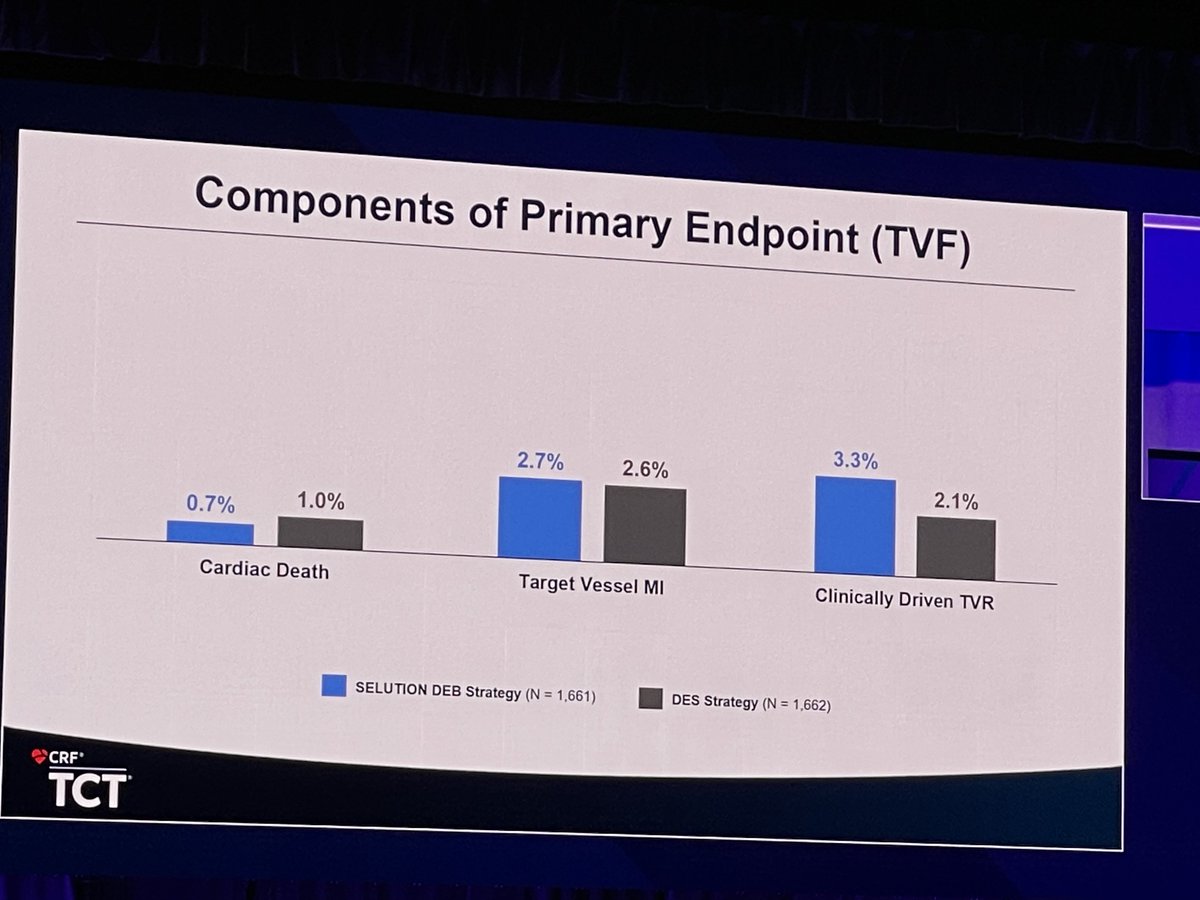
@jonnywatt @evandrofilhobr Ok so you have to trade off a slightly higher 1 year repeat revasc rate for SEB against a slightly higher cardiac death rate in DES
Death is undoubtedly the ultimate endpoint.
A repeat revasc is a choice…
Time to start making choices
English