Aldo Letelier retweetledi
Aldo Letelier
1.3K posts

Aldo Letelier
@aldolete
Neurólogo Vascular HCVB, Valparaiso, V Región #utachcvb [email protected]
Viña del Mar, Chile Katılım Mart 2011
4.4K Takip Edilen1.4K Takipçiler


Aldo Letelier retweetledi



Aldo Letelier retweetledi

📲🧠The Stroke Riskometer™ App improved stroke knowledge compared to usual care group at 6 months
📉Lacked evidence for retaining knowledge at 12 months
Read more about the app here👇
journals.sagepub.com/doi/abs/10.117…

English
Aldo Letelier retweetledi

Feeling bipolar about bilateral thalamic lesions?
Unfortunately, the differential for bilateral thalamic lesions isn’t binary!
But here’s an easy mnemonic to help: THALAMIC!
T = Tumor (glioma)
H = Hypoxic/ischemic encephalopathy
A = Artery of Percheron Infarct
L = Loss of thiamine (Wernicke’s)
A = ADEM
M = Metabolic/Toxic
I = Internal cerebral vein thrombosis. Infection (west nile)
C = Creutzfeld-Jacob
Now you’ll never bypass a bilateral thalamic diagnosis with this easy mnemonic!

English
Aldo Letelier retweetledi

Insisto mucho en los beneficios de caminar aunque sean 10 minutos después de comer.
Es algo sencillo, pero que de verdad cambia tu vida.
Un ensayo aleatorizado publicado en Scientific Reports (2025) comparó caminar 10 minutos inmediatamente después de comer frente a una caminata de 30 minutos y frente a no moverse.
Resultado: solo 10 minutos reducen el pico de glucosa en sangre de forma significativa, igual de eficaz que 30 minutos. La línea de puntos es el control (sin caminar). Las otras dos son 10 y 30 minutos. La diferencia habla sola.
El mecanismo es simple: el músculo activo capta glucosa directamente sin necesitar insulina. Menos pico, menos bajón de energía a las 3 de la tarde, menos grasa acumulada a largo plazo.
Después de comer, 10-15 minutos andando. Sin teléfono si puedes. Es el hábito más barato y más infrautilizado que existe para controlar el azúcar y la energía del día.
Fuente estudio: PubMed.

Español
Aldo Letelier retweetledi

Reversible cerebral vasoconstriction syndrome: A narrative review
CCR Journal Watch
criticalcarereviews.com/latest-evidenc…

English
Aldo Letelier retweetledi

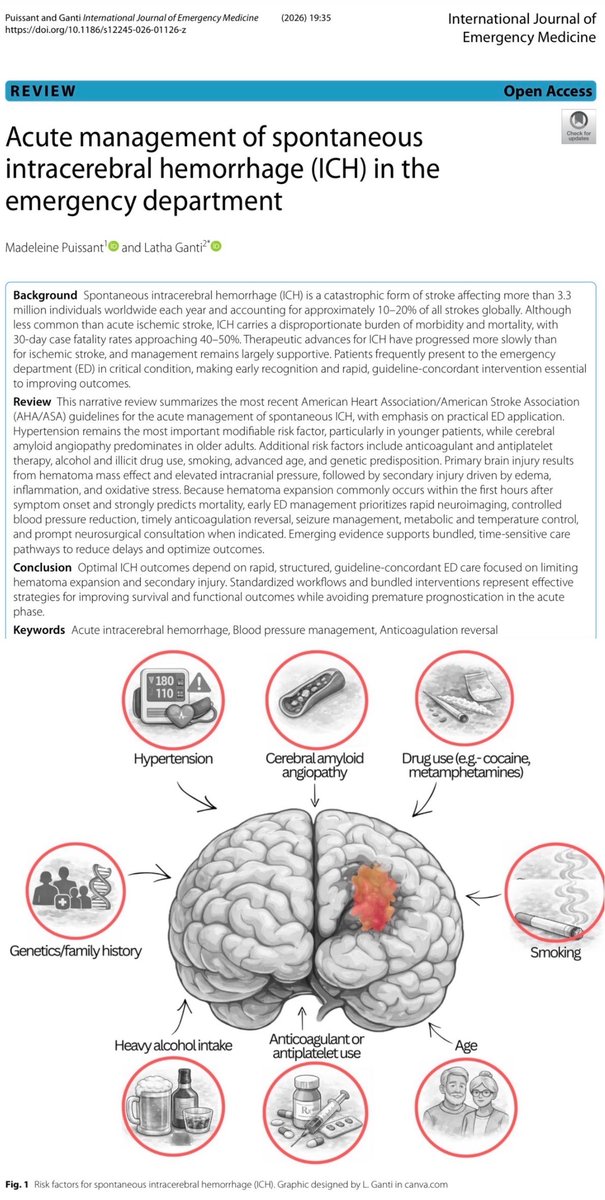
🩸🧠 𝗛𝗜𝗖 𝗲𝘀𝗽𝗼𝗻𝘁𝗮́𝗻𝗲𝗮 𝗲𝗻 𝗨𝗿𝗴𝗲𝗻𝗰𝗶𝗮𝘀: “𝗖𝗢𝗗𝗘 𝗜𝗖𝗛” 𝘆 𝗹𝗮 𝗵𝗼𝗿𝗮 𝗱𝗲 𝗼𝗿𝗼 ⏱️🚨
@BioMedCentral
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
t.me/ClubCrit
⬇️⬇️⬇️⬇️
🧵👇
📌La HIC es devastadora (≈10–20% de los ictus) y con letalidad alta (≈40–50% a 30 días) 😰. Lo que más impacta en ED/UCI es 𝙚𝙫𝙞𝙩𝙖𝙧 𝙚𝙭𝙥𝙖𝙣𝙨𝙞𝙤́𝙣 𝙙𝙚𝙡 𝙝𝙚𝙢𝙖𝙩𝙤𝙢𝙖 en las primeras horas 🔥🧠.
🛟 𝘼𝘽𝘾 + 𝙣𝙚𝙪𝙧𝙤𝙚𝙭𝙖𝙢𝙚𝙣 𝙧𝙖́𝙥𝙞𝙙𝙤: 𝙚𝙨𝙩𝙖𝙗𝙞𝙡𝙞𝙯𝙖 𝙮 𝙘𝙪𝙖𝙣𝙩𝙞𝙛𝙞𝙘𝙖 🧠📏
✅ A/B/C primero (intuba si no protege vía aérea o GCS ≤8) 🫁💉
🎯 Objetivo SpO₂ >94% 🌬️✅
🧠 Examen + escalas: 𝙂𝘾𝙎, 𝙉𝙄𝙃𝙎𝙎 𝙮 𝙄𝘾𝙃 𝙨𝙘𝙤𝙧𝙚 para severidad y comunicación con neuro/neurocirugía 📞🧠.
🩻⚡ 𝙄𝙢𝙖𝙜𝙚𝙣: 𝙏𝘼𝘾 𝙨𝙞𝙣 𝙘𝙤𝙣𝙩𝙧𝙖𝙨𝙩𝙚 𝙥𝙧𝙞𝙢𝙚𝙧𝙤 (𝙮 𝘾𝙏𝘼 𝙨𝙞 𝙖𝙥𝙤𝙧𝙩𝙖) 🧠🩻
🟦 𝙉𝘾𝘾𝙏 confirma HIC, localiza, estima tamaño, IVH, hidrocefalia y shift 🧭
📌 Hematoma grande = peor pronóstico; HE ocurre temprano (hasta 1/3) ⏱️
🟠 𝘾𝙏𝘼 puede detectar causa secundaria y el “𝙨𝙥𝙤𝙩 𝙨𝙞𝙜𝙣” (extravasación) → predice expansión y peor outcome 🎯🩸.
📉🧯 𝙋𝙧𝙚𝙨𝙞𝙤́𝙣 𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡: 𝙗𝙖𝙟𝙖𝙧 “𝙨𝙪𝙖𝙫𝙚 𝙮 𝙨𝙤𝙨𝙩𝙚𝙣𝙞𝙙𝙤”🎢🚫
HTA persistente = más expansión y peor evolución 😬
🎯 Guía AHA: iniciar control 𝙚𝙣 𝙡𝙖 𝟭ª 𝙝𝙤𝙧𝙖, ideal con 𝙞𝙣𝙛𝙪𝙨𝙞𝙤́𝙣 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙖 (nicardipina/labetalol) 💉
✅ Objetivo 𝙋𝘼𝙎 𝟭𝟰𝟬 y mantener 𝟭𝟯𝟬–𝟭𝟱𝟬
🚫 Evitar caídas >60 mmHg en la 1ª hora
🚫 Evitar PAS <130 en HIC leve–moderada si llega con PAS >150 (parece dañino)
🧬🩸 𝙍𝙚𝙫𝙚𝙧𝙨𝙞𝙤́𝙣 𝙙𝙚 𝙖𝙣𝙩𝙞𝙘𝙤𝙖𝙜𝙪𝙡𝙖𝙘𝙞𝙤́𝙣: “𝙙𝙚𝙣𝙩𝙧𝙤 𝙙𝙚 𝙡𝙖 𝟭ª 𝙝𝙤𝙧𝙖” ⏱️🧯
La anticoagulación aumenta hematoma, expansión y mortalidad 😱 → reversión precoz salva cerebro 🧠
🟣 𝘼𝙑𝙆 (𝙬𝙖𝙧𝙛𝙖𝙧𝙞𝙣𝙖): Vit K 10 mg IV + 𝟰𝙁-𝙋𝘾𝘾 (meta INR ≤1.4; incluso INR 1.3–1.9 considerar PCC) ✅
🟠 𝙓𝙖 𝘿𝙊𝘼𝘾 (𝙖𝙥𝙞𝙭/𝙧𝙞𝙫𝙖/𝙚𝙙𝙤𝙭): 𝟰𝙁-𝙋𝘾𝘾. 𝘈𝘯𝘥𝘦𝘹𝘢𝘯𝘦𝘵 mostró mejor control de expansión pero fue retirado del mercado US (dic 2025) ⚠️
🔵 𝘿𝙖𝙗𝙞𝙜𝙖𝙩𝙧𝙖́𝙣: 𝙞𝙙𝙖𝙧𝙪𝙘𝙞𝙯𝙪𝙢𝙖𝙗; si no hay, considerar PCC y/o TRR selectiva 🫘
🟢 𝙃𝙚𝙥𝙖𝙧𝙞𝙣𝙖/𝙇𝙈𝙒𝙃: protamina 💉
🌡️🍬⚡ 𝙁𝙞𝙚𝙗𝙧𝙚, 𝙜𝙡𝙪𝙘𝙤𝙨𝙖 𝙮 𝙘𝙧𝙞𝙨𝙞𝙨: 𝙡𝙤 “𝙥𝙚𝙦𝙪𝙚𝙣̃𝙤” 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙢𝙖𝙩𝙖 🧠🔥
🌡️ Fiebre 1º 72h (30–45%) = peor pronóstico → tratar hipertermia puede ser razonable ✅ (hipotermia no recomendada rutina)
🍬 Hiperglucemia (hasta 60% en 24h) = peor outcome → tratar hipo/hiper; umbral práctico >180–220 mg/dL ⚠️
⚡ Convulsiones 4–42% (24–72h): si clínica/EEG → tratar inmediato ✅; profilaxis sin evidencia de crisis NO rutinaria 🚫
🧠🧯 𝙄𝘾𝙋/𝙄𝙑𝙃 + 𝙣𝙚𝙪𝙧𝙤𝙘𝙞𝙧𝙪𝙜𝙞́𝙖 (𝙥𝙧𝙞𝙢𝙚𝙧𝙖𝙨 𝟮𝟰𝙝) 🚨
🧠 Si ↑ICP: bolos hiperosmolares (HTS preferida) como puente; 𝙀𝙑𝘿 salva vidas en hidrocefalia obstructiva 🧠🧊
🔪 Cirugía: considerar temprano (MISTIE III sugiere beneficio mortalidad en algunos; cerebelosa ≥15 mL + deterioro/compresión = intervenir) 🧠🔧
📦 “Bundled care” tipo 𝘾𝙊𝘿𝙀 𝙄𝘾𝙃:
➡️ Reversión
➡️ PA
➡️ Glucosa
➡️ Temperatura
➡️ Neurocirugía
✅ Mejora outcomes 🧩✅
🛑 Y clave humana: 𝙚𝙫𝙞𝙩𝙖𝙧 𝙙𝙚𝙘𝙞𝙨𝙞𝙤𝙣𝙚𝙨 𝙙𝙚 𝙡𝙞𝙢𝙞𝙩𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙨𝙤𝙥𝙤𝙧𝙩𝙚 𝙚𝙣 𝙡𝙖𝙨 𝙥𝙧𝙞𝙢𝙚𝙧𝙖𝙨 𝟮𝟰𝙝 (incertidumbre pronóstica) ⏳🧠.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [clubcrit.wordpress.com]
#Neurocritical #NeuroX #NeuroICU #Neurology #ICH #Emergencias #Radiology #Stroke #Hypertension #Anticoagulation #PatientSafety #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #POCUS #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada



Español

"Aurora: Open-Access Web Application for Structured Neuroradiology Report and Score Calculation"
doi.org/10.3174/ajnr.A…
@alexandraseugi

English

Aldo Letelier retweetledi


Aldo Letelier retweetledi

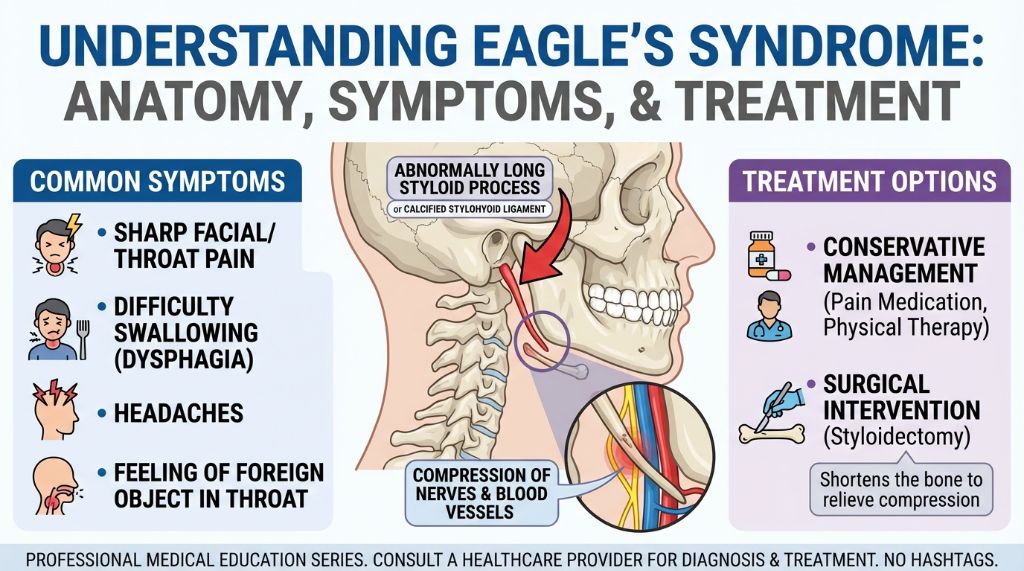
Eagle Syndrome: An elongated styloid process or calcified stylohyoid ligament causes this rare condition.
It manifests as chronic head, neck, and throat pain.
Nerve and blood vessel compression are key factors.
Symptoms include sharp pain, dysphagia, headaches, and globus sensation.
Diagnosis involves imaging to visualize the styloid process.
Treatment ranges from analgesics and physical therapy to styloidectomy.
English
Aldo Letelier retweetledi

The callosal angle in possible iNPH assessment is measured on a coronal plane perpendicular to the anterior commissure-posterior commissure line, at the level of the posterior commissure.
The technique is demonstrated erroneously in this #journalimage
doi.org/10.1056/NEJMra…

English
Aldo Letelier retweetledi
When do you restart anticoagulation after stroke?
Maybe this piece from @StrokeAHA_ASA might help
ahajournals.org/doi/full/10.11…
English
Aldo Letelier retweetledi

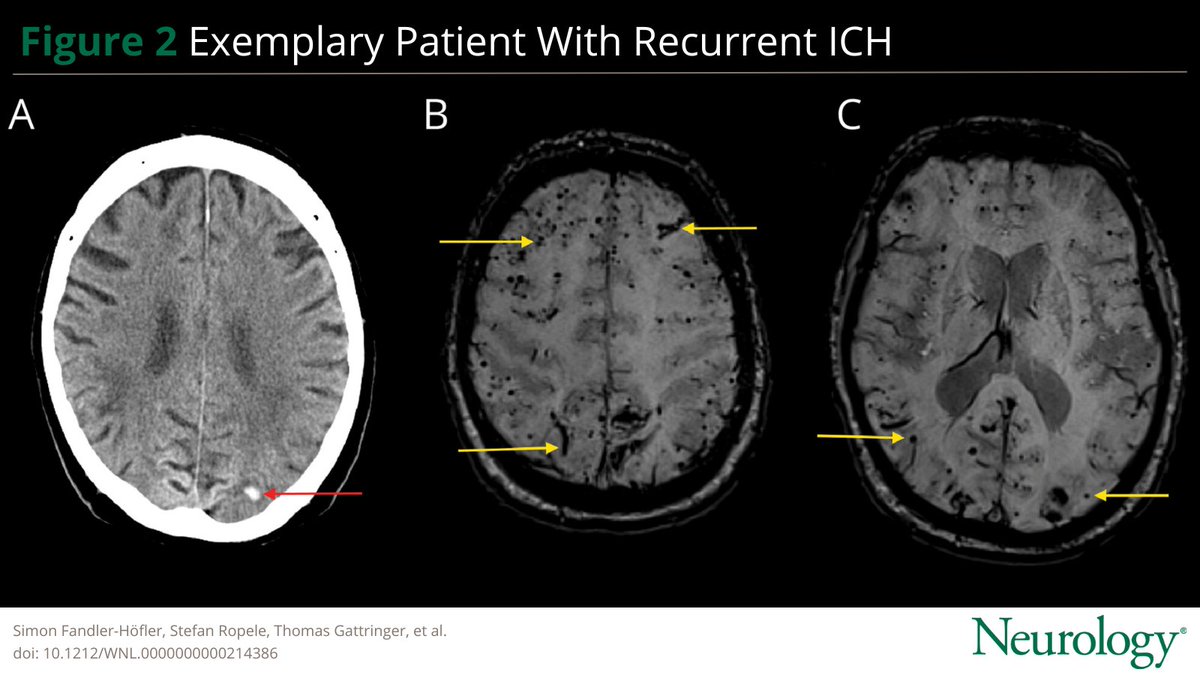
In this study the authors assessed the role of neuroimaging in identifying patients with particular susceptibility to #IschemicStroke or intracerebral hemorrhage, with the potential to enable individualized risk stratification: hubs.la/Q03V_lDq0
#NeuroTwitter @SimonFaHo
English
Aldo Letelier retweetledi
🫀Meta-analysis finds PFO closure is associated with a ⬇️reduced risk of recurrent stroke compared to antithrombotic therapy alone in patients over 60
🔎Most studies were observational - more RCTs needed
Read more here👇
journals.sagepub.com/doi/full/10.11… @behnam_jazayeri

English
Aldo Letelier retweetledi

In this target trial emulation study, Levetiracetam was more effective than Valproic Acid for preventing Poststroke Seizures neurology.org/doi/10.1212/WN…
English
Aldo Letelier retweetledi

Fighter Pilot Syndrome: A Bow Hunter Syndrome Variant Identified With Dynamic Cerebral Angiography | Stroke: Vascular and Interventional Neurology ahajournals.org/doi/full/10.11… @SVINJournal @svinsociety @StrokeAHA_ASA

English
Aldo Letelier retweetledi

New publication from the Cardiology Experts Team at The Meta-Analysis Academy, and it’s in JACC! Congratulations to Nelson, Guilherme, and all collaborators.
It’s truly rewarding to see The Meta-Analysis Academy alumni achieving such great success!
jacc.org/doi/10.1016/j.…
#Cardiology #JACC #MedTwitter

English
Aldo Letelier retweetledi