
dontlikethis
122 posts



Ultras? None can test my viral capture of Melville Street’s
bambini pazzi
vm.tiktok.com/ZNR9SoyJy/
English
dontlikethis retweetledi

"And I said to the horse...."
1974 📸 John Drysdale

English

Hey Good Looking......What You Got Cooking?
A Spanish Tortilla - to be served with a tomato and anchovy salad

English
@roisinmurphy @_ConnieShaw right I thought! Let's hear what these nasty women have to say- and then listening to each one of them I wept every day for about 3 months. I was shattered and shocked to hear what had been going on.
English
@roisinmurphy @_ConnieShaw After getting into trouble for not understanding what JK Rowling had said wrong and hearing about Nazis at parliament (likely FWS) my friend posted proof of JK being a Nazi- a photo with Kathleen Stock, Julie Bindel and a bunch of other normal looking ladies....
English

On the contrary, ‘transphobia’ is as a result of educating yourself so much you almost wish you hadn’t
nyara@nyaraVT
Transphobia is a refusal of educating yourself on trans topics because it makes you feel strong when you can weaponise your ignorance to harm the powerless. It is also extremely profitable.
English
dontlikethis retweetledi

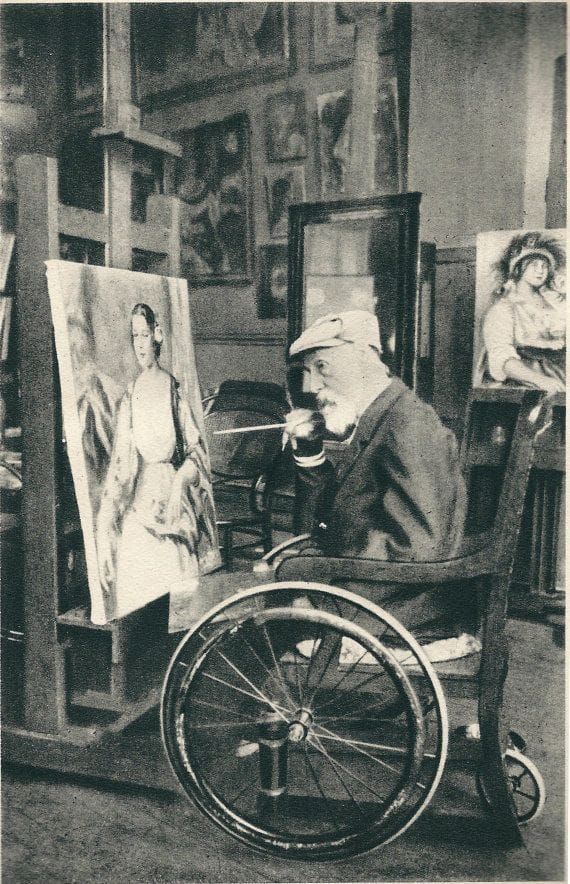
The arthritic and wheelchair-bound Renoir still painting, 1914.
English
@roisinmurphy @_ConnieShaw I was in turmoil for years after 'educating' myself. I had absolutely no idea how awful things had become.
English

@_ConnieShaw “Get educated!!” Backfires completely. Trust me I know..
English
dontlikethis retweetledi


dontlikethis retweetledi

DRUG CONSUMPTION ROOMS WERE AN EXPERIMENT.
THE RESULTS ARE NOW IN. Edinburgh is being asked to believe something very simple.
That a supervised drug consumption room will reduce harm, tidy up the streets, and quietly guide people into treatment and recovery.
It sounds compassionate. It sounds reasonable.
It is also, at this point, no longer an untested idea.
Because this exact model, often in more expansive forms, has already been tried across parts of North America. And we now have the benefit of something policy rarely waits for.
Outcome.
The most comprehensive analysis comes from Professor Keith Humphreys at the Brookings Institution, examining drug policy reforms across the Pacific Northwest between 2020 and 2024. What followed the shift toward decriminalisation, reduced enforcement, and expanded harm reduction was not what had been promised.
Overdose deaths rose, in some places to record levels.
Crime and public disorder increased.
Open drug use became more visible, more normalised, and more embedded in everyday spaces.
This was not a marginal change. It was a visible shift in how entire neighbourhoods functioned.
The argument had been that removing pressure would lead people toward help. That if you made drug use safer, people would be more likely to seek treatment.
In practice, that simply did not happen.
In Oregon, after decriminalisation, more than 90 percent of people given a route into treatment ignored it. The system spent thousands per call trying to engage people, with almost no measurable movement into care.
In San Francisco, a flagship centre designed to “link” people into treatment managed to refer roughly one in three hundred users.
That is not a pathway. That is a policy built on hope rather than behaviour.
Even where harm reduction was most developed, the results were no better. British Columbia, with one of the most extensive systems in the world including supervised consumption and safe supply, recorded its highest ever overdose death rates in successive years.
If this model were going to work anywhere, it would have worked there.
It didn’t.
And this is where the debate stops being abstract.
Because these policies do not exist in a vacuum. They change the environments around them.
They concentrate drug use into specific areas.
They anchor dealing to place.
They normalise behaviours that were once hidden.
Residents begin to see what was previously out of sight. Businesses adapt or leave. Public spaces change their character.
We are already hearing early versions of this in Glasgow. Reports of discarded needles. Public injecting. A death outside the facility.
Again, not an outlier. A pattern.
Now, there will always be those who say this is the cost of compassion. That saving lives in the moment justifies everything else.
But even that claim does not stand as cleanly as it once did.
Peer-reviewed research has found no clear reduction in overdose deaths following decriminalisation in Oregon and Washington. Government audits have described systems that failed to deliver meaningful treatment access. Journalists, clinicians, and even former advocates have begun to acknowledge the gap between promise and reality.
And perhaps most telling of all, the communities who lived under these policies have begun to reject them.
San Francisco voters removed the officials who led the shift.
Oregon repealed its flagship decriminalisation law.
Washington reintroduced penalties.
British Columbia has begun reversing course on public drug use.
This is not ideology. This is lived experience turning into democratic response.
Because people will entertain theory. They will not tolerate living indefinitely inside its consequences.
And beneath all of this sits a harder truth that policy language tends to obscure.
Without clear pathways into treatment, recovery and reintegration, policy stops confronting addiction and begins accommodating it. It attempts to stabilise and manage a condition that, by its very nature, cannot be stabilised or managed. If addiction could be controlled, it would not be addiction at all. What follows is not care but containment, a quiet acceptance that some lives will be indefinitely parked on the margins so long as death is delayed.
That is the real trade being offered.
Less visible overdoses inside a facility, in exchange for more visible addiction outside it.
Less immediate risk, in exchange for less long-term change.
So when Edinburgh’s leaders say this will “benefit the city as a whole,” the question is not whether the intention is good.
The question is whether the evidence supports it.
Because we are no longer guessing.
We have already run the experiment.
And the results are not what was promised.
Annemarie Ward 💜@Annemarieward
THEY SAY IT WILL “BENEFIT THE CITY” HERE’S WHAT HAPPENED WHERE THEY TRIED IT @TheScotsman #Edinburgh #DrugConsumptionRoom #Consultation We’ve heard the script before. A supervised drug consumption room will reduce harm. It won’t attract more users. It will clean up public spaces. It will connect people into treatment. It will “benefit the city as a whole.” That is exactly what is now being proposed for Edinburgh’s Old Town. But before anyone signs off on this, we need to do something radical in public policy. We need to look at what actually happened elsewhere. Not theory. Not intentions. Outcomes. Because the most detailed real-world test of these ideas has already taken place across the Pacific Northwest of North America between 2020 and 2024. Cities like San Francisco, Portland, Seattle and Vancouver implemented versions of the same approach Edinburgh is now being asked to accept. The result was not what was promised. According to Professor Keith Humphreys’ Brookings report “The Rise and Fall of Pacific Northwest Drug Policy Reform” , what followed was a sharp and visible deterioration in both public safety and addiction outcomes. brookings.edu/wp-content/upl… Start with the core claim. That reducing enforcement and expanding harm reduction would reduce deaths and stabilise communities. It didn’t. Overdose deaths rose to record levels across the region. Oregon and Washington saw some of the fastest increases in fatal overdoses in the entire United States. British Columbia reached its highest ever death rates despite having one of the most extensive harm reduction systems in the world. That alone should give pause. But it didn’t stop there. Crime and disorder increased sharply in many of these cities. Violent crime rose by double digits in places like San Francisco, Oregon and Washington, while property crime surged well above national trends. And perhaps most telling of all, public drug use became normalised in everyday spaces. Humphreys describes how streets that were once busy with ordinary life became dominated by open drug use, dealing, and street disorder, particularly as policing retreated and public spaces emptied. Now pause for a moment and compare that to what residents near Glasgow’s Thistle Centre are already reporting. A “carpet of drug paraphernalia.” Needles. Syringes. A death outside the facility. That is not an outlier. That is the pattern. Because here is the uncomfortable truth that policymakers avoid saying out loud. These facilities do not exist in isolation. They reshape the surrounding environment. They anchor drug markets to specific locations. They normalise public injecting. They change who uses the space and how it is used. And once that shift happens, it is very difficult to reverse. Then there is the question Edinburgh officials keep gently implying but never quite answering. Do these services move people into recovery? Again, we have real-world data. In Oregon, more than 90 percent of people given the option to engage with treatment simply ignored it. The system spent thousands per phone call trying to connect people, with almost no measurable movement into care. In San Francisco, a flagship “linkage centre” that was supposed to connect people to treatment ended up referring roughly 1 in 300 users. That is not a pathway. That is a holding pattern. And here is where the moral question cuts through the policy language. Without clear pathways into treatment, recovery and reintegration, policy stops confronting addiction and begins accommodating it. It attempts to stabilise and manage a condition that, by its very nature, cannot be stabilised or managed. If addiction could be controlled, it would not be addiction at all. What follows is not care but containment, a quiet acceptance that some lives will be indefinitely parked on the margins so long as death is delayed. That is the trade being offered. Less visible overdoses inside a building, in exchange for more visible addiction outside it. Less pressure to change, in exchange for more tolerance of decline. And crucially, this is not just an academic debate anymore. The public in those same cities eventually rejected these policies. San Francisco recalled its district attorney. Oregon repealed its flagship decriminalisation law. Washington reintroduced penalties. British Columbia began reversing course on public drug use. Why? Because people will tolerate theory. They will not tolerate living in it. They saw what happened to their streets, their businesses, their parks, and their sense of safety. And they voted accordingly. So when Edinburgh’s leaders say this will “benefit the city as a whole,” the question is simple. Based on what evidence? Because the best available real-world evidence tells a very different story. And once these facilities are in place, once the geography of drug use shifts, once the norms change, it is not a pilot anymore. It is a direction of travel. The question for Edinburgh is not whether the intention is compassionate. The question is whether the outcome will be. And on the evidence we already have, that is a hard no. The Humphreys paper gives you the system-level collapse story. What you want alongside it are pieces that show three things clearly. First, that decriminalisation and harm-reduction-heavy models have not reduced deaths. Second, that engagement with treatment does not automatically follow. And third, that communities experience real, measurable impacts. Let me walk you through the strongest, credible sources you can lean on. Start with the one you already have in your archive, above because it is gold dust in this debate. The Atlantic piece by Keith Humphreys and Rob Bovett on Oregon’s decriminalisation failure. It is not ideological. It is forensic. Full article: theatlantic.com/ideas/archive/… What it shows, plainly, is that removing penalties did not lead to treatment engagement. Over 90 percent of people issued citations ignored them. The system created a theoretical pathway to help, but almost nobody walked down it. That is the key point you can hammer. Access is not the same as uptake. Policy can offer help, but addiction does not politely accept invitations. Then bring in the official Oregon audit, because nothing lands harder than a government admitting failure in its own words. Oregon Secretary of State Audit (2023): sos.oregon.gov/audits/Documen… This is devastating in tone. It describes a system that was poorly implemented, slow to fund services, and unable to demonstrate meaningful outcomes. Even sympathetic readers cannot escape the conclusion that the infrastructure simply wasn’t there to support what was promised. Now, if you want to broaden beyond the US and avoid the predictable “that’s America” dismissal, British Columbia is your strongest parallel to Scotland. British Columbia Coroners Service reports (ongoing): www2.gov.bc.ca/gov/content/li… Despite one of the most extensive harm reduction systems in the world, including safe supply and supervised consumption, overdose deaths reached record highs year after year. That is the uncomfortable contradiction. If harm reduction alone were sufficient, BC should be the global success story. It isn’t. Then there is the Washington Post reporting on Portugal, which is important because Portugal is constantly used as the moral shield for these policies. washingtonpost.com/world/2023/07/… The key takeaway is not that Portugal “failed”, but that its success depended on something almost always omitted in UK debates. Strong social pressure, family structures, and crucially, dissuasion mechanisms that still push people towards treatment. It was never a free-for-all. It was structured, culturally embedded, and backed by intervention. Strip those out, and you are not copying Portugal. You are caricaturing it. Then bring in the academic angle, because critics will ask for peer-reviewed evidence. JAMA Psychiatry study on Oregon and Washington (2023): pubmed.ncbi.nlm.nih.gov/37755815/ This study found no clear reduction in overdose deaths following decriminalisation. Not an increase necessarily, but crucially, no improvement. That alone undermines the central promise. And finally, if you want something that speaks directly to community impact, Brandon del Pozo’s analysis is worth using because it comes from someone who straddles policing and public health. Boston Globe opinion: bostonglobe.com/2024/04/25/opi… His core point is brutally simple. Harm reduction began as a population health strategy, but policy drift meant the wider public was effectively removed from the equation. When communities feel ignored, policy loses legitimacy, no matter how well-intentioned it is. Now step back and look at the pattern across all of this. No consistent evidence of reduced deaths. Weak or negligible engagement with treatment. Rising public disorder in multiple settings. Eventual political backlash from the very communities expected to accept it. That is not a fringe critique. That is a convergence of data, audits, journalism, and lived outcomes. The debate is no longer about whether these policies are compassionate in theory. The question is whether they work in practice, and whether they respect the communities expected to live with them. Because once you widen the lens beyond a single press release or consultation document, the evidence is no longer neat, and it is certainly not reassuring.
English
dontlikethis retweetledi

In 1933, visionary choreographer Busby Berkeley stunned audiences with one of the most spectacular musical sequences ever filmed in the classic pre-Code movie Footlight Parade.
English
dontlikethis retweetledi

Swans have one of the coolest water landing techniques ever
English
dontlikethis retweetledi

QUINTUPLETS 🐑🐑🐑🐑🐑
We can't remember having quintuplets before on the farm so this was a special moment ✨
#sheep365 #familyfarm #lambing2026

English
dontlikethis retweetledi

'Bathed in Gold' Taken shortly after sunrise this morning, walking down from Glastonbury Tor. I can never resist just one more photograph before I leave.

English
dontlikethis retweetledi

dontlikethis retweetledi
dontlikethis retweetledi


dontlikethis retweetledi
dontlikethis retweetledi


dontlikethis retweetledi
Now compare that with treatment.
Residential rehabilitation in Glasgow costs about £1,200 per week, or roughly £171 per day. For less than the price of one supervised visit, someone can receive a full day of structured therapy, clinical support and recovery work designed to help them stop using drugs altogether.
In plain terms, Scotland is currently paying more to manage the risks of addiction than it would cost to actively treat it.
Read more theglasgowsplash.substack.com/p/exclusive-th…
English