Sabitlenmiş Tweet
.
8.4K posts


.
@aminergic
Internal Medicine 🩺 || Dakhni - Kannadiga (دکھنی - ಕನ್ನಡಿಗ) || Random musings on whatnot across the space time continuum...
Karnataka Katılım Kasım 2014
319 Takip Edilen231 Takipçiler



. retweetledi
Came across this interesting book on Dakhni sayings by Prof Zabiulla. Here are some of my favorites. 🧵

English

. retweetledi

Anticoagulation therapy is the foundation of acute PE management. Use of DOACs and LMWH allow for rapid and predictable anticoagulation therapy in most patients with acute PE. Further management strategies are dictated by individual risk factors for adverse events. These include the measurement of biomarkers, RV size and function on imaging, and hemodynamics.
Informed by these risk factors, decisions can be made about the utility of advanced interventions, including catheter-directed thrombolysis, mechanical thrombectomy, surgical embolectomy, and extracorporeal membrane oxygenation. Use of a PERT to facilitate decision-making around acute interventions is recommended.
✍🏼 @GoldbergJBCTMD @Dkadiandodov @RosovskyRachel @sabeedak1 @hjcox_pvd @JunLiMD @mnyoung1

English
Baelor's entrance in support of Ser Duncan as the theme plays on, going down as one of the best scenes in the GoT universe.
GIF
.@aminergic
Watching Dunk and Egg is much enjoyable than House of the Dragon.
English
@stupidydumdum That's so true. The eminence it once held has faded (It never regained since the fall of the Adil Shahis in 1680s) and only the remnant monuments are the witness to the bygone era. Although it is a Tier 3 city, the region deserves much more attention.
English
@aminergic Oh, sorry. I thought you were saying "Kittur-Karnataka". 😅
I agree, however, Bijapur makes me sad, considering what it was in it's heyday.
English
Yes and let that be in districts of NE/ Kalyana Karnataka.
Kiran Mazumdar-Shaw@kiranshaw
To realize Karnataka's full potential, development must extend to other cities, creating widespread #employment opportunities, strengthening the state's growth story, and reducing overconcentration in #Bengaluru.
English
@stupidydumdum I'd say Raichur and Gulbarga. Hubli Dharwad is well enough relatively.
English
Apart from the books,
Life in the fast lane website.
Dr. Tanmay Bhandari@TanmayB21431752
I am 1 month into medicine residency. I need help with mastering ECGs. Please share your best resources for learning ECGs.
English
. retweetledi

🚨I don’t comment on every tech launch, but after eight years in healthcare AI, I have to ask: is India handing over its healthcare sovereignty to foreign platforms? 🇮🇳
I must share some raw thoughts about the launch of ChatGPT Health (for patients) and OpenAI for Healthcare (for doctors) this week, because the implications are enormous, and we as Indians need to pay attention (which we aren’t!)
In the last 24 hours, OpenAI has initiated a direct play to become the “operating system” for global healthcare data. This is not just about replacing human doctors but about becoming the default interface where your health data, wearables, lab reports, clinical notes, fitness logs (and literally everything related to you) gets stored, organized, interpreted and ultimately monetized!
🚀 Healthcare is now one of the world’s biggest data economies. In India, this market is exploding, well over 500 billion dollars, with digital health leading the way.
In India have more than a billion people (and potential customers). The diversity of cases we see in hospitals is unmatched! TB, rheumatic heart disease, tropical infections, cancers all of them present differently in Indian populations. A treasure trove of clinical information that does not exist anywhere else in the world!
And for decades, most of this data has been siloed and stuck in different places. Fitness apps stored your steps and activity. Hospitals locked up imaging in their PACS. Half our X-rays and ultrasounds are still physical films or printouts lol
AI has changed everything in the last few years.
Today, models can read scans, parse clinical notes, integrate vitals, understand behavior, and connect it all. We have patient health record apps which store all our information, so it’s easier for us to connect them to AI apps through APIs and MCP servers.
The truth is: Whoever controls the layer that stitches this together will control diagnostics, healthcare policy, and population health at scale. I have absolutely no doubt about that!
That is what OpenAI is building. Connect your records. Connect your wearables. Let the platform learn how your body, your disease, your life works. It starts free. Later, you pay for the smarter version.
We have seen this movie before. Google Drive. iCloud. Google Photos. Once your data and your habits live inside a system, how do you ever leave? Right?
But healthcare is not just your email or photos. There is sovereign angle to it. If India’s imaging, clinical records, and behavioral data flow only into foreign platforms, (and yes, many Indian startups have already been forced to share data just to survive), we are reduced to data suppliers, not data owners, and definitely not builders.
If this continues it will be disastrous!!! Our diagnostic standards. Our clinical pathways. Our public health priorities. All of it may eventually be shaped by decisions made outside this country!
I see something every day in practice. Indian TB. Rheumatic heart disease. Infections and patterns Western models still struggle to understand. If we allow foreign entities to own the “brain” trained on this data, we will end up paying for insights generated from our own people.
I have worked, often pro bono, with some of the most brilliant health-tech founders in this country. They are hardworking, creative, deeply committed. But most are just fighting for survival. No one has the runway to build national infrastructure!
An Indian “ChatGPT for Health” cannot be another under-funded startup. We need patient capital. Serious policy support. Digitization of decades of legacy records. Multimodal datasets that connect hospitals, labs, public systems, wearables, and wellness platforms. Long-term governance that balances privacy, equity, and innovation.
And I am not being anti-global. This is not anti-free market. And honestly, anyone who reduces this to that is missing the point!
We absolutely need global collaboration. But the core intelligence built on Indian health data MUST be governed in India.
Because The stakes are massive.
Whoever controls health data and health AI will set the rules for medical care, public policy, and healthcare innovation for the next decade.
If we build our own now, we control our future.
If we wait, we will be locked out and locked in.
The clock is ticking.
So my question is: Are we going to do something about it, or are we going to remain passive users while a few companies in Silicon Valley decide how healthcare for 1.4 billion Indians should work?


English
. retweetledi

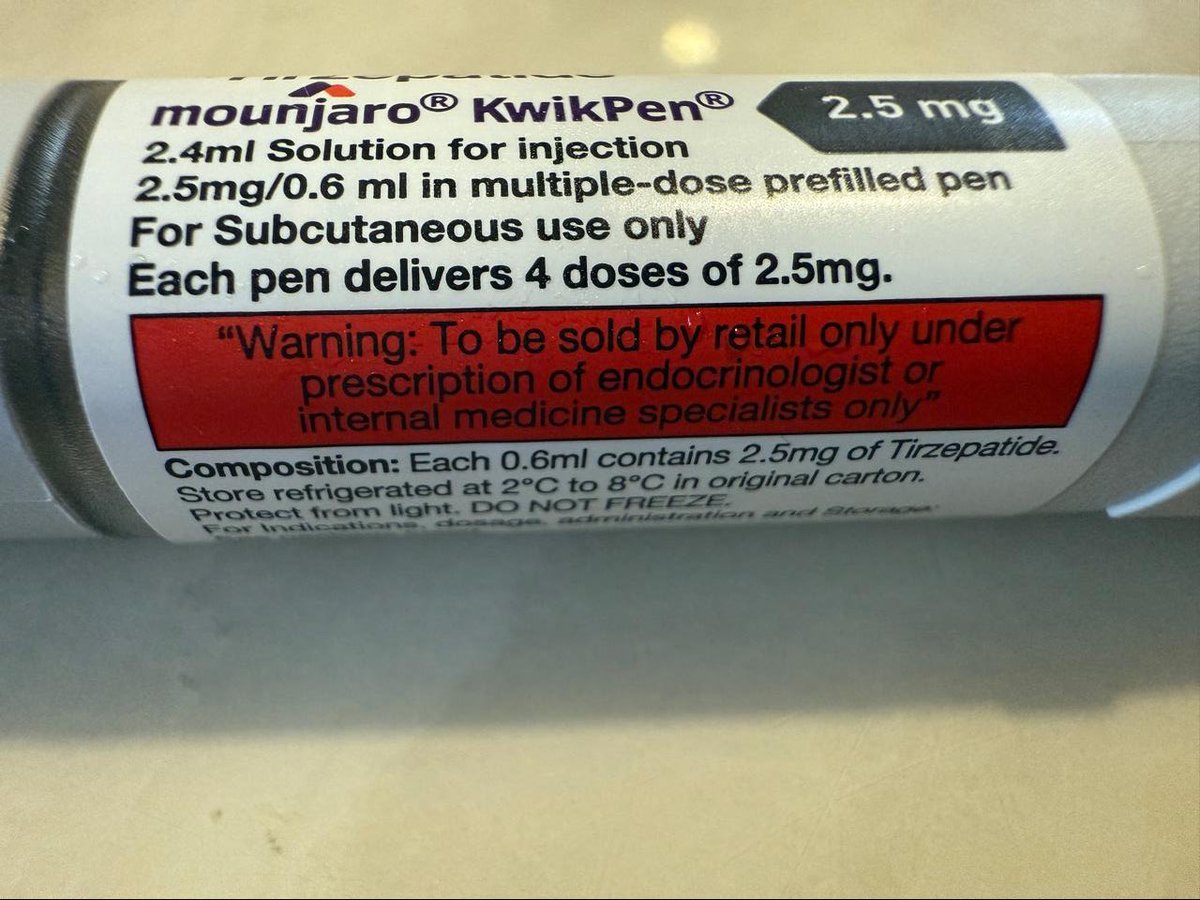
Mounjaro packaging is very clear:
Prescription only by endocrinologists & internal medicine specialists.
So no - your trainer, influencer, or beautician does not count as healthcare.
Followers ≠ medical degree.
English

With 55 wickets in 3 world cups('15, 19, 23), Shami is the all time highest wicket taker for India in the world cups. Only an arrogant and stupid selector would keep him out of the squad.
IndiaToday@IndiaToday
Fast bowler Mohammed Shami was not recalled to India’s ODI squad for the 3-match ODI series against New Zealand. Despite consistent performances in the domestic season, Shami was overlooked as the selectors opted for Mohammed Siraj, Arshdeep Singh, Harshit Rana and Prasidh Krishna as the preferred fast-bowling quartet in the 50-over format. Shami’s personal coach lashed out at the selection call and slammed chairman of selectors Ajit Agarkar after the squad was announced. Speaking to India Today over the phone, the coach vented his frustration and questioned what more the pacer could do to force his way back into the Indian side. #MohammedShami #Shami #Coach #AjitAgarkar #ITCard
English
. retweetledi

It's very very important that u r surrounded by non medico Friends or people around u just to know life exists without studies, medicines and tensions!
#MedTwitter
English
