Amolo Chris retweetledi
Amolo Chris
1.2K posts

Amolo Chris
@amolo_chris
love for medicine and service to humanity
Nakuru, Kenya Katılım Aralık 2018
228 Takip Edilen67 Takipçiler


Amolo Chris retweetledi

🚨Nitrofurantoin is ineffective in pyelonephritis because it does not achieve therapeutic concentrations in renal parenchyma or blood.
Explanation
Nitrofurantoin is rapidly excreted into urine
It attains high urinary concentrations
But has poor tissue penetration and low serum levels
👉 Therefore, it is effective for lower UTIs (cystitis) but not for upper UTIs (pyelonephritis), which involve renal parenchyma and often systemic infection.
Key pharmacologic reasons
1. Poor renal tissue penetration
2. Inadequate serum concentration
3. No efficacy in bacteremia, which commonly accompanies pyelonephritis
Exam / guideline pearl
> Nitrofurantoin: cystitis only — never pyelonephritis or urosepsis
What to use instead (examples)
Fluoroquinolones (e.g., ciprofloxacin, levofloxacin)
Third-generation cephalosporins
Piperacillin–tazobactam (severe cases)
Bottom line:
Nitrofurantoin treats urine, not kidney tissue hence ineffective in pyelonephritis.
English
Amolo Chris retweetledi

Pharmacotherapy of Atrial Fibrillation (AF)
Management is built on 3 pillars:
1️⃣ Rate control: β-blockers or non-DHP CCBs (EF > 40%); digoxin as adjunct or alternative; IV amiodarone in critically ill or HFrEF
2️⃣ Rhythm control: antiarrhythmic selection guided by structural heart disease and LVEF; anticoagulation required peri-cardioversion
3️⃣ Stroke prevention: CHA₂DS₂-VASc-based anticoagulation; DOACs preferred over warfarin except in mechanical valves or mod-severe MS
English
Amolo Chris retweetledi

Which drug is used to treat serotonin syndrome.? 🤔

English
Amolo Chris retweetledi

Audi Q5 S-line TFSI
Year 2018
2.0L I4 Turbocharged Petrol DAXB
252 bhp
Quattro AWD
7-speed DSG
Milleage 62,000kms
WAUZZZFY8J2212954
Panoramic sunroof
Multifunctional steering wheel
Paddle shifters
Electronically adjustable seats
Electronic tailgate
Heated leather seats
Reverse camera
Electronic handbrake
Parking sensors front and rear
Auto hold
Wireless charger and USB ports
360° surround view
Price 6,200,000ksh
📍 Mombasa
☎️📥 +254 729 233495




Nyali, Kenya 🇰🇪 English
Amolo Chris retweetledi

🌊SEVERE RHEUMATOID ARTHRITIS (RA)
🤹The image shows classic advanced RA deformities, including:
🌀 Ulnar deviation at MCP joints
🌀 Swan-neck deformities (PIP hyperextension + DIP flexion)
🌀Boutonnière deformities (PIP flexion + DIP hyperextension)
🌀 Joint subluxation & ligament laxity
🌀 Symmetrical involvement — hallmark of RA
🤹Why RA causes these deformities?
•🌀Chronic autoimmune inflammation → synovial hypertrophy (pannus)
•🌀Pannus erodes cartilage, bone & tendons
•🌀Extensor tendons slip ulnarward → ulnar deviation
•🌀Imbalance between flexor–extensor forces → swan-neck/boutonnière patterns
•🌀Repeated inflammation → permanent joint remodeling
🧑⚕️Important Investigations:-
•🛡️RF (Rheumatoid factor) – positive in ~70–80%
•🛡️Anti-CCP antibodies – highly specific
•🛡️Raised ESR/CRP
•🛡️X-ray → periarticular osteopenia, joint space narrowing, marginal erosions
🧑⚕️Treatment Essentials:-
🛡️1. DMARDs
•Methotrexate (first-line)
•Leflunomide, Sulfasalazine, Hydroxychloroquine
🛡️2. Biologics
•Anti-TNF (Etanercept, Adalimumab)
•IL-6 inhibitors (Tocilizumab)
•JAK inhibitors (Tofacitinib)
🛡️3. Steroids
•For acute flares only
🛡️4. Physiotherapy
•Prevents stiffness & progression
#RheumatoidArthritis #Autoimmune #JointDeformity #MedFacts #MedStudents #Rheumatology #ClinicalMedicine #KriMeeraPharma
Dr Ihab Suliman@IhabFathiSulima
What is the diagnosis 💔⁉️
English
Amolo Chris retweetledi

💠Behcet's Disease- It is a rare, chronic vasculitic disorder involving multiple systems.
📍C/F- Classic triad= Recurrent oral & genital ulcers, erythema nodosum, uveitis.
✓ Dx- Hallmark - Pathergy reaction- it is a heightened skin response to trauma.
• When the skin is pricked with a sterile needle, a papule or pustule develops at the site of prick within 24-48 hrs in patients with Behcet's disease.
📍T/t- Symptomatic, supportive. No specific cure.
English
Amolo Chris retweetledi
🟡Spironolactone is used in cirrhotic ascites as 1st-line therapy due to antagonism of secondary hyperaldosteronism, promoting natriuresis while sparing potassium.
∆ Mechanism-It is an Aldosterone antagonist, blocks Na+ reabsorption/ENaC in cortical collecting duct leading to Increased urinary Na+ excretion (diuresis)& K+ retention (prevents hypokalemia from loop diuretics).
∆ Advantages over Loops Diuretics- Physiologic (targets cause), single agent effective in 90%, less metabolic disturbance.
English
Amolo Chris retweetledi
Yes, overuse of inhalers like salbutamol can make asthma attacks more frequent over time.
🔴Excessive use (>2 times a week or >12 canisters/year) is linked with increased risk of asthma exacerbations, hospitalizations & even death.
∆ Mecanism- Downregulation & desensitization of beta-2 receptors, reducing responsiveness to bronchodilators & increasing airway inflammation.
• Overuse drives airway hyperreactivity & can result in paradoxical bronchospasm.
• Over-reliance on SABAs may mask poor asthma control & delay use of controlller therapy (inhaled corticosteroids).
∆ Associated metabolic effects- Tachycardia, hypokalemia, tremors, anxiety & lactic acidosis may occur in overdose.
English
Amolo Chris retweetledi
🟡3% Hypertonic Saline is preferred over Mannitol for lowering ICP because of-:
• Greater & longer-lasting ICP reduction.
• Better cerebral perfusion.
• Less risk of hypovolemia & electrolyte disturbance.
∆ Mannitol remains widely used but needs close monitoring for volume status.
∆ Choice depends on clinical context, but Hypertonic Saline is gaining favor especially in traumatic brain injury & refractory ICP cases.
English
Amolo Chris retweetledi

🌊In burn patients, the BEST IV fluid to prevent acidosis is → Ringer Lactate (RL).
🤹Why RL?
🌀Normal Saline causes hyperchloremic metabolic acidosis due to high chloride load.
🌀Ringer Lactate contains lactate → converted to bicarbonate, helping buffer acidosis.
🌀RL closely mimics extracellular fluid → better volume resuscitation + fewer electrolyte shifts.
🌀D5W & 3% saline are not used for burn resuscitation.
🤹Clinical Pearl:
Use Parkland Formula for burn resuscitation:
4 mL × kg × %TBSA (first 24 hours) — half in first 8 hrs.
#BurnCare #EmergencyMedicine #Acidosis #FluidTherapy #MedTwitter #MedicalEducation #TraumaCare #KrimeeraPharma
English
Amolo Chris retweetledi

🛑 Transudate vs Exudate (Effusion)
📌 Transudate:
🔷️ Low protein (<3 g/dL)
🔷️ Low LDH
🔷️ Due to pressure imbalance (HF, cirrhosis)
🔷️ Clear, watery fluid
📌 Exudate:
🔷️ High protein (>3 g/dL)
🔷️ High LDH
🔷️ Due to inflammation (TB, pneumonia, cancer)
🔷️ Cloudy, thick fluid.

English
Amolo Chris retweetledi

#ER #ED
What is the diagnosis?
What is the first step in the management ?
#MEDHM #MedX @IhabFathiSulima

English
Amolo Chris retweetledi

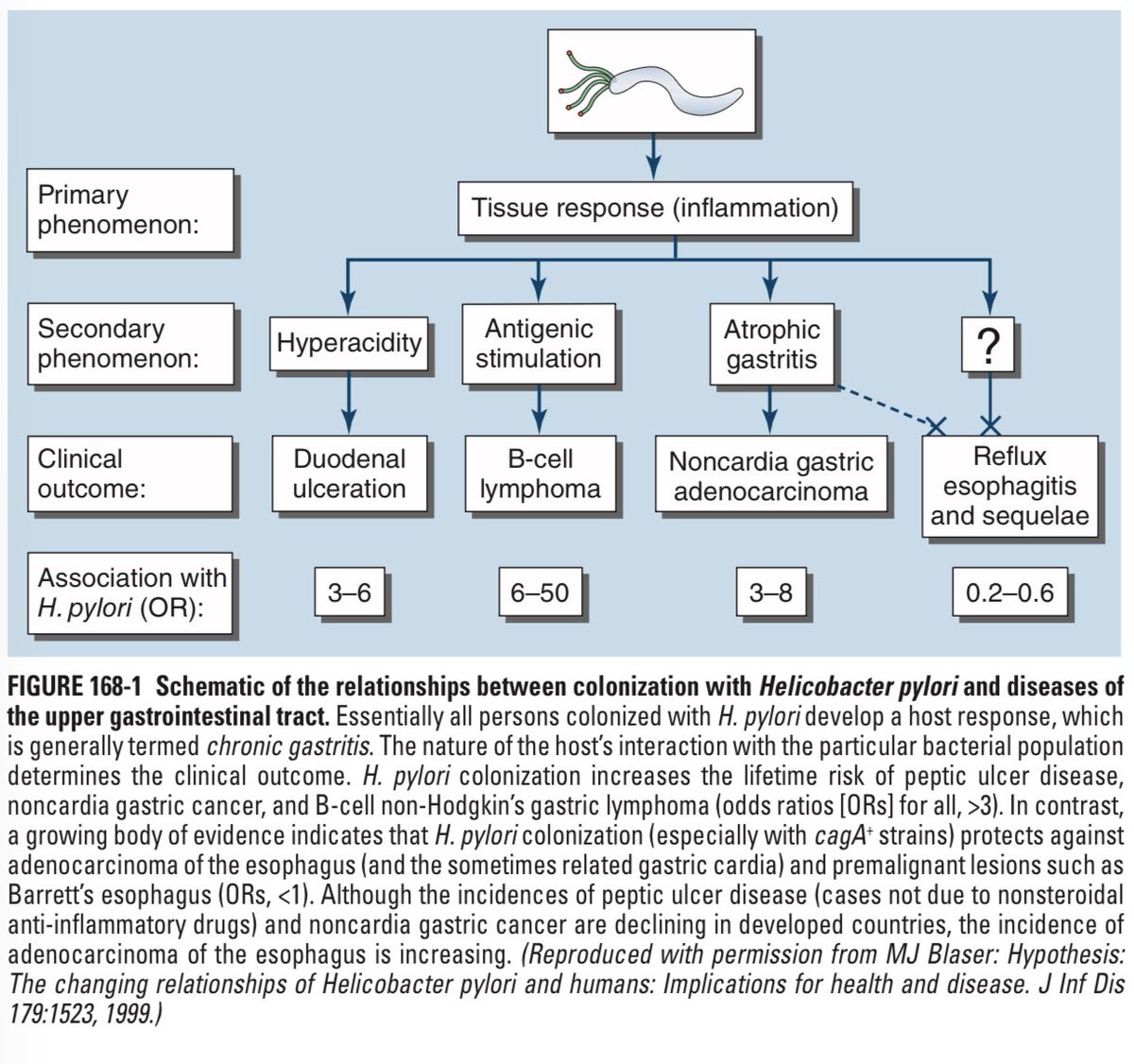
🧫 H. pylori
It infects billions.
It hides in acid.
It causes ulcers, anemia, lymphoma, and even cancer.
Yet in some people, it protects against reflux.
This is the strange story of Helicobacter pylori, one of the most impactful microbes in human history.
👨⚕️ A discovery that changed medicine
Before 1982, ulcers were blamed on stress and spicy food.
Then two Australian doctors, Barry Marshall and Robin Warren, made history.
Marshall swallowed a flask of bacteria, developed gastritis, and proved that H. pylori was the real cause.
That single experiment won them the 2005 Nobel Prize and forever changed gastrointestinal medicine.
🦠 What exactly is H. pylori
A gram-negative, spiral-shaped, flagellated bacterium that thrives inside your stomach.
Nearly 40% of the global population carries it, usually acquired during childhood.
Once it settles in, it often stays for life unless eradicated.
🔥 What it does to your stomach
Every infected person develops chronic gastritis, but most remain symptom-free.
A smaller group develops ulcers or even cancer depending on where the bacteria live.
📍 Infection in the antrum increases gastrin and acid secretion, causing duodenal ulcers.
📍 Infection in the corpus decreases acid production, leading to gastric ulcers and gastric cancer.
The location of infection decides the disease.
⚙️ How it causes damage
🧬 CagA damages stomach cells and raises cancer risk.
💥 VacA creates toxic pores in the cell membrane.
🧫 Urease protects it from acid.
CagA-positive strains are especially linked with ulcers and malignancy.
🩺 Diseases linked to H. pylori
✅ Peptic Ulcer Disease (duodenal and gastric)
✅ Gastric Adenocarcinoma
✅ Gastric MALT Lymphoma (can regress after eradication)
✅ Functional Dyspepsia
✅ Iron Deficiency Anemia
✅ Idiopathic Thrombocytopenic Purpura
😲 The paradox of protection
Some studies suggest that long-term H. pylori infection may protect against
•GERD
•Barrett’s Esophagus
•Esophageal Cancer
The reason is reduced acid output, which limits reflux.
But this mild protection never outweighs the risk of ulcers and gastric cancer.
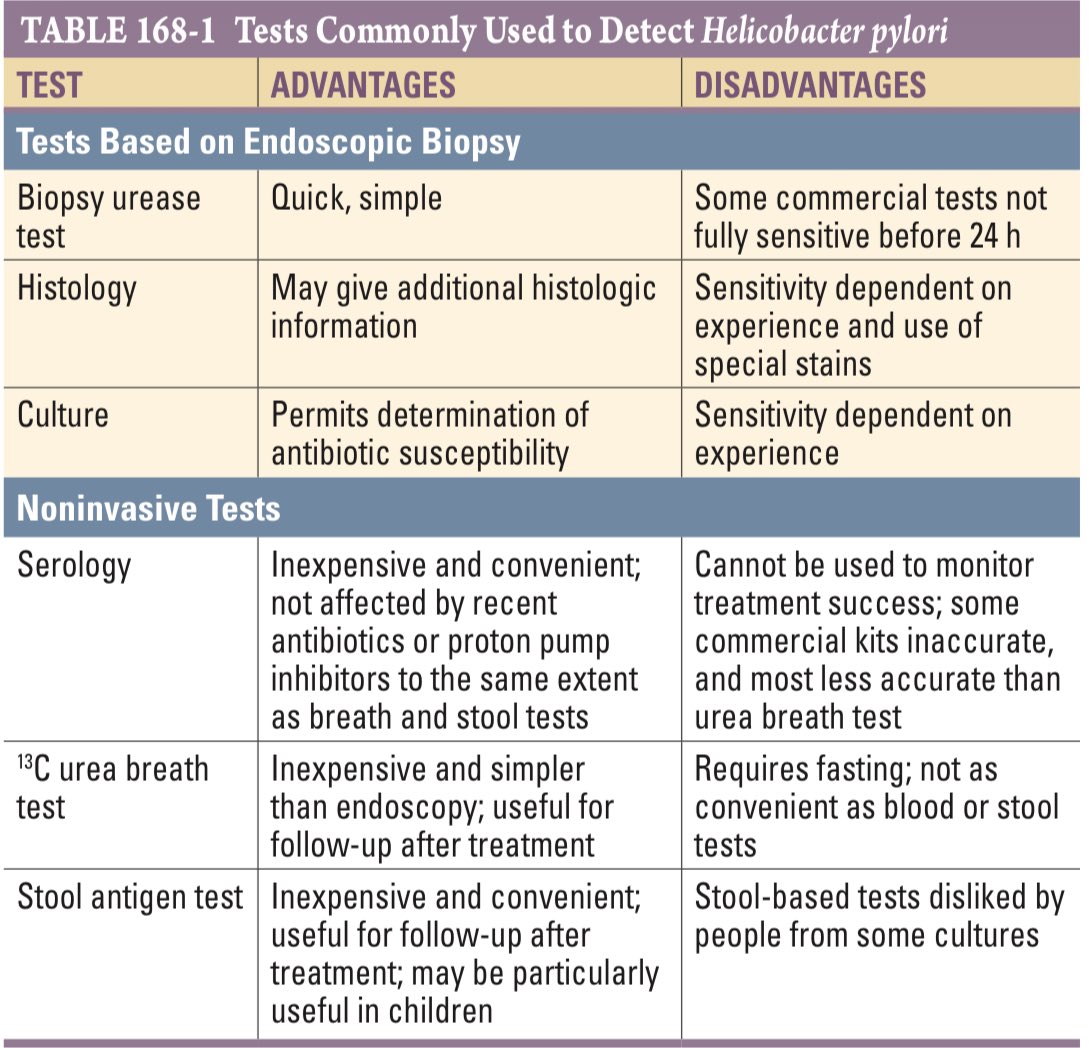
🔬 How to diagnose it
🫧 Urea Breath Test : most accurate for diagnosis and follow-up
💩 Stool Antigen Test : inexpensive and reliable
🩸 Serology (IgG) : shows exposure, not active infection
During endoscopy, doctors may also perform
•Biopsy with rapid urease testing
•Histology
•Culture for resistant strains
⏳ The “test of cure” rule
Always confirm eradication.
Perform the urea breath test or stool antigen test at least 4 wks after completing therapy.
Stop PPIs for 2 wks and antibiotics or bismuth for 4 wks before testing.
Testing too early can give a false negative result.
💊 When to treat
Treatment is strongly indicated in:
✅ Peptic ulcer disease (active or healed)
✅ Gastric MALT lymphoma
✅ Functional dyspepsia
✅ ITP or unexplained iron or vitamin B12 deficiency (consider)
Routine treatment of healthy carriers is not recommended because of antibiotic resistance concerns.
💥 How to treat it
Treatment always requires combination therapy.
Two or more antibiotics with a proton pump inhibitor for 10 to 14 days.
High-dose PPIs improve eradication.
Success depends on adherence and local resistance rates.
Preferred regimens in 🇮🇳
🧩 Bismuth Quadruple Therapy
PPI + Bismuth + Tetracycline + Metronidazole
🧩 Concomitant Quadruple Therapy
PPI + Amoxicillin + Clarithromycin + Tinidazole
Clarithromycin-based triple therapy should be avoided in areas with high resistance.
🧬 If the first regimen fails
Try a different combination such as Levofloxacin-based therapy.
Never repeat the same failed regimen.
If infection persists after two courses, culture the organism and choose antibiotics based on sensitivity testing.
⚠️ Common mistakes to avoid
❌ Testing too early after antibiotics
❌ Using PPIs before testing
❌ Repeating failed regimen
❌ Skipping test of cure
🔚 Like ❤️ and Repost 🔁
👉 Follow @DrNikhilMD


English
Amolo Chris retweetledi

Duodenal atresia
Why?
Two large bubbles: one gastric, one proximal duodenal, separated by a constricted pyloro-duodenal region.
Little/absent gas distally beyond the second bubble → indicates an obstruction at the duodenum.
Typical neonatal chest/abdomen radiograph shows this pattern strongly suggesting duodenal atresia.
English
Amolo Chris retweetledi

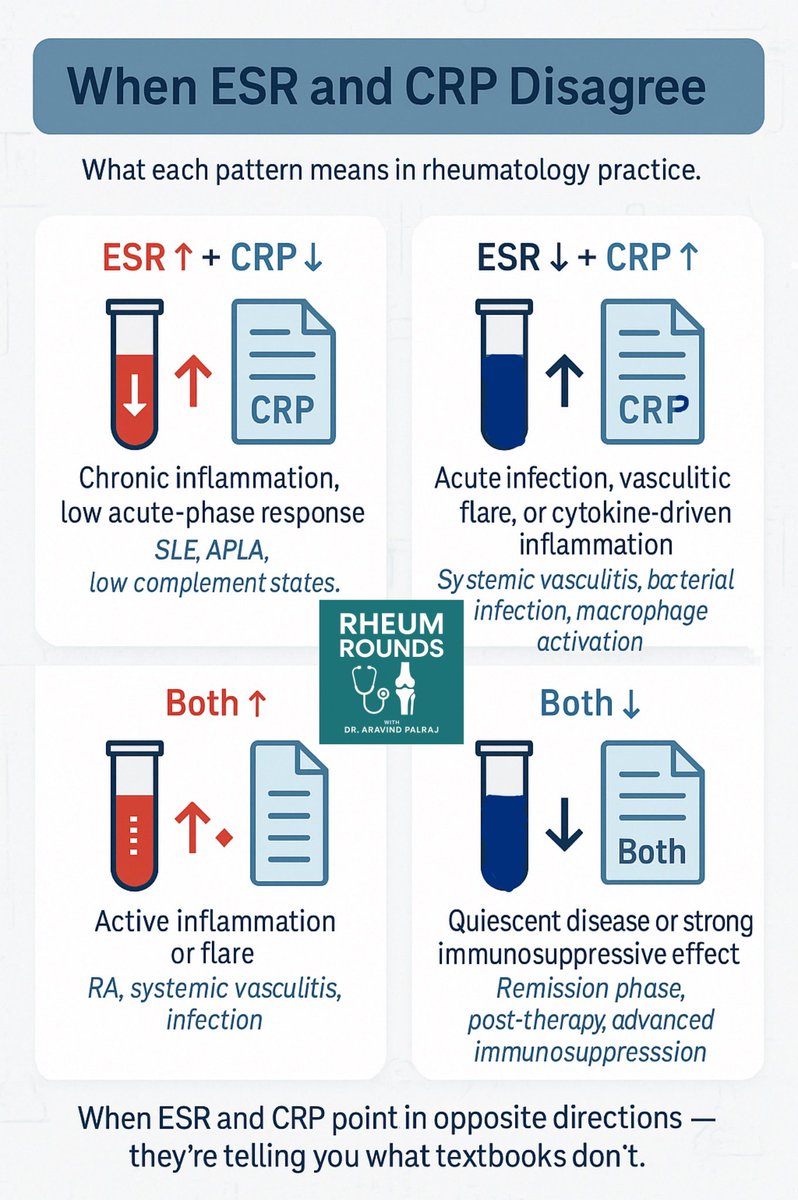
When ESR and CRP disagree, your job isn’t just to record numbers —
it’s to interpret what the body’s really saying.
🧪 ESR ↑ + CRP ↓ → SLE, APLA
🧪 ESR ↓ + CRP ↑ → Infection, Vasculitis
🧪 Both ↑ → Flare
🧪 Both ↓ → Remission
They don’t lie — they whisper clues.
👇 Save this infographic.
#Rheumatology #MedTwitter #FOAMed #ClinicalPearls #MedEd @DrAkhilX @IhabFathiSulima @CelestinoGutirr @ArunInamadar @Janetbirdope
Aravind Palraj@Rheumat_Aravind
🧵 Thread: ESR vs CRP – Friends? Foes? Or Just… Different? They’re both inflammatory markers—but they don’t always agree. Let’s break down how they differ, overlap, and mislead. #MedTwitter @IhabFathiSulima @DrAkhilX @CelestinoGutirr
English
Amolo Chris retweetledi

The bird’s beak sign of achalasia refers to the tapered narrowing of the distal esophagus seen on a barium swallow (esophagram) — it looks like a bird’s beak pointing toward the stomach.
🧠 Explanation:
In achalasia, there is loss of inhibitory neurons (NO and VIP) in the myenteric (Auerbach) plexus, leading to:
Failure of lower esophageal sphincter (LES) relaxation
Loss of peristalsis in the esophageal body
As a result, food and fluid accumulate above the LES → proximal esophageal dilation with a narrow, smooth taper at the gastroesophageal junction → the bird’s beak appearance.
🔍 Radiologic features:
Dilated proximal esophagus (fluid level may be seen)
Smooth, symmetric tapering distally
No mucosal irregularities (helps distinguish from carcinoma)
🧪 Diagnostic confirmation:
Barium swallow → “Bird’s beak” sign
Manometry → Increased LES tone + absent peristalsis
Endoscopy → To exclude malignancy (pseudoachalasia)
💊 Management:
Pharmacologic: Nitrates, calcium channel blockers (short-term relief)
Definitive:
Pneumatic dilation
Heller myotomy
Botulinum toxin injection (temporary, elderly patients)
English
Amolo Chris retweetledi
✴️Piperacillin + Tazobactam is commonly given to most hospitalized patients because-:
• Piperacillin is a broad-spectrum β-lactam antibiotic that inhibits bacterial cell wall synthesis by binding to penicillin-binding proteins (PBPs), leading to bacterial cell death.
• Many bacteria produce β-lactamase enzymes that degrade β-lactam antibiotics like piperacillin, causing resistance.
∆ Tazobactam is a β-lactamase inhibitor that protects piperacillin from degradation by irreversibly inhibiting these enzymes, restoring & extending piperacillin's antibacterial spectrum.
∆ This combination effectively targets a wide range of gram-positive, gram-negative, aerobic & anaerobic bacteria, including many β-lactamase producing hospital pathogens.
📍It is especially useful for severe, polymicrobial infections common in hospitalized patients, such as intra-abdominal infections, respiratory tract infections, skin & soft tissue infections & febrile neutropenia.
English
Amolo Chris retweetledi
🔴 Activated charcoal is given within 1 hour of toxin ingestion because-:
∆ Activated charcoal works by adsorbing toxins in the gastrointestinal tract, preventing their absorption into the bloodstream.
• Adsorption is most effective when administered early (within 1 hour) because the toxin is still in the stomach or intestines & can be bound by charcoal.
• The large surface area of activated charcoal alllows binding of many drugs & poisons, reducing their bioavailability & systemic toxicity.
• It also interrupts enterohepatic & enteroenteric circulation of some toxiins, aiding in their elimination.
📍Activated charcoal is not effective against all poisons (e.g., alcohols, metals like iron and lithium, acids and alkalis).
English
Amolo Chris retweetledi

Brain Death
Brain death is clinically defined as follows:
• No pupillary, corneal, gag, or oculocephalic reflexes
• No response to stimuli
• Absence of drug intoxication, hypothermia, hypotension
Brain death is confirmed with apnea testing, not a scan or neurologist
consult. To test for apnea:
1. Oxygenate the patient for 20 minutes.
2. Disconnect patient from the ventilator.
3. Measure pCO2.
A pCO2 level increase of ≥20 shows apnea and confirms brain death.
English