English
Dr. Seto
25 posts




I think we can advise patients that with low SYTAX score (and especially low functional SYNTAX score) the data suggests better outcomes with PCI and more similar to those with CABG. #CardsJC
@CardioNerdsJC We know we can only limit this to hypothesis generation since its a subgroup analysis, but i believe this line of thought is echoed by SYNTAX #CardsJC

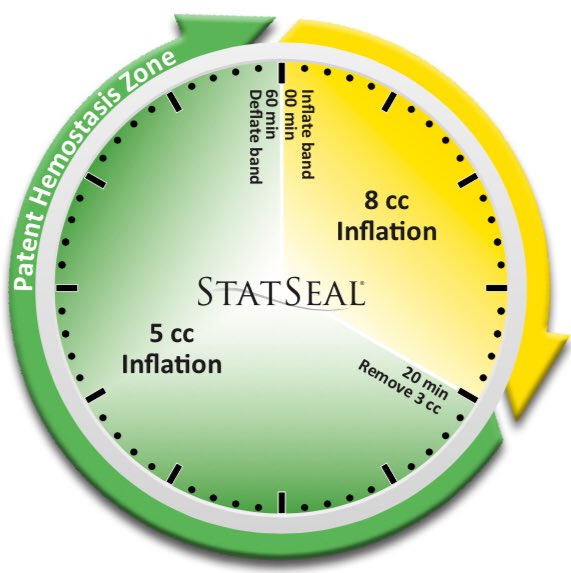
SCAI Consensus Statement for Length of Stay after PCI. Dr. Seto and Dr. Boudoulas outline the top takeaways from #SCAI2018 cardiologynownews.org/scai-consensus… @SCAI @BaimInstitute @arnoldseto @KDBoudoulas twitter.com/CMichaelGibson…