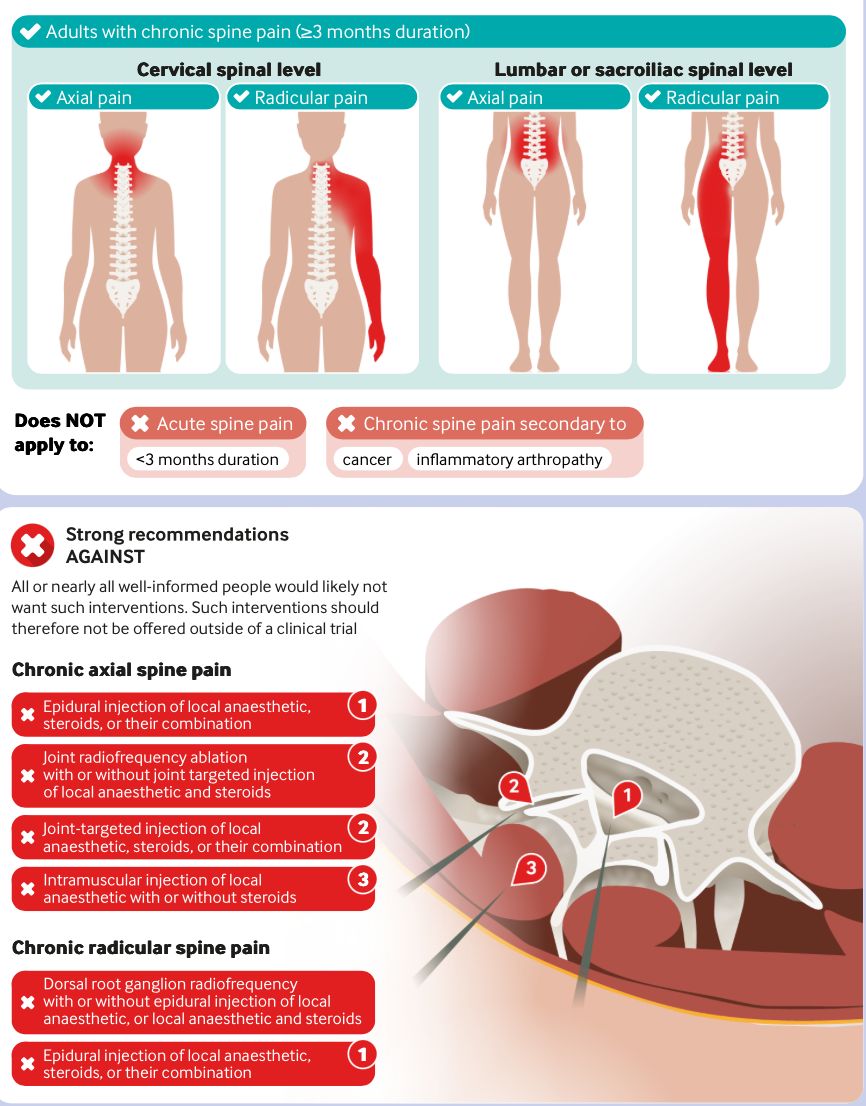
Spinal injections 💉 strongly NOT recommended for chronic back, neck and sacroliliac pain ⛔️
Here's a 🧵 on the recent (and controversial) BMJ study and why I think some caution is needed here.
Does marathon running increase arthritis risk? A recent study of 3,804 runners would suggest not!
There are limitations; arthritis prevalence was determined by asking runners if they'd been diagnosed with it by a doctor. See full paper for details DOI: 10.1177/19417381231190876
Truly superb work by @rtenews RTE Investigates on the appalling state of psychiatric care in Ireland.
We really, really need to address these issues.
Public broadcasting at its finest.
I wrote this on X yesterday: Bending from the knees (instead of the back) ruined a generation. Now they’re giving horrible advice to the next generation.
It was an experiment. I was curious where people would go with this.
When I wrote it... I wasn’t saying technique doesn’t matter. And I wasn’t saying people should lift recklessly.
I was pointing out how a coaching cue became a fear-based rule—and how that rule shaped how people think about their bodies. Fear grips people today. In my office people fear movement patterns, jumps, hops, stairs etc and always have a reason... I have X,Y or Z. When in fact... X,Y and Z would feel better if they trained properly.
“Lift with your knees, not your back” became “Never lift with your back.”
Over time, it became dogma.
The implicit message people absorbed wasn’t about load management or skill.
It was this: your spine is fragile.
And that idea stuck.
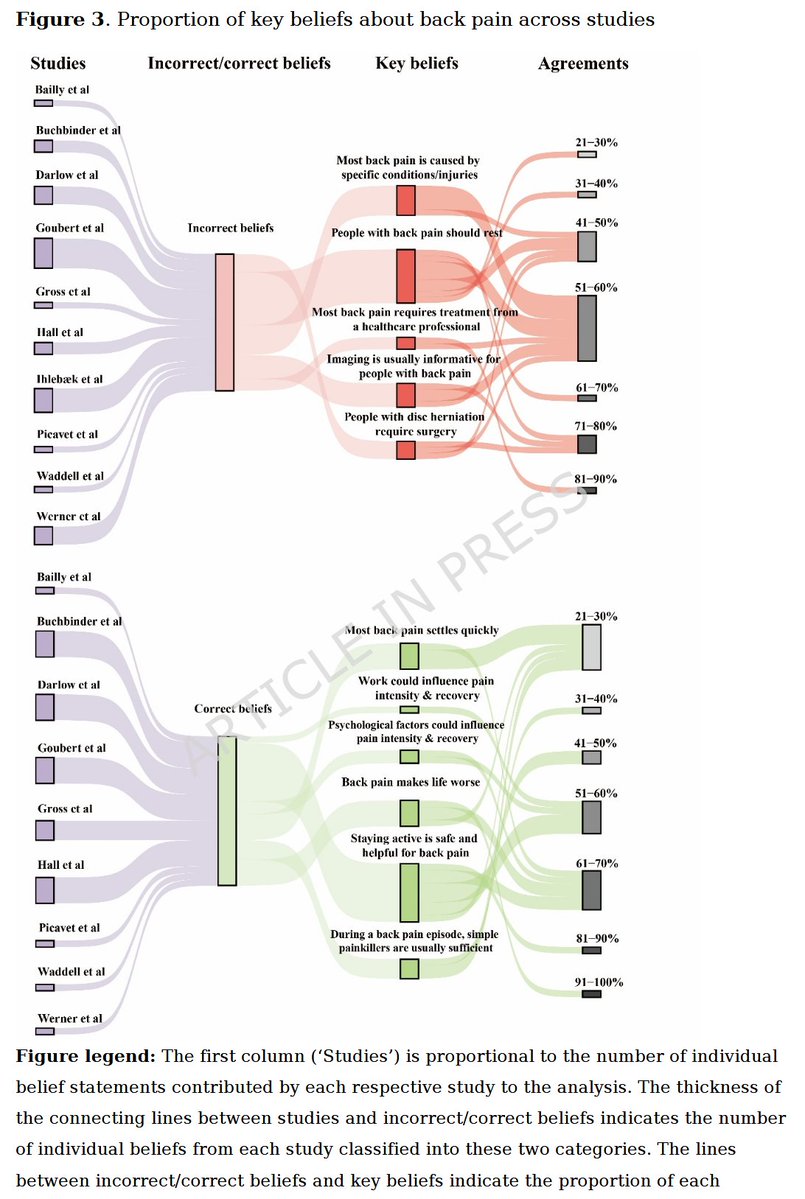
Many said there's data to support this... well... not really.
There is no high-quality randomized controlled trial evidence showing that teaching people to lift “with their knees instead of their back” reduces injury risk.
None.
This has been studied extensively in occupational health and ergonomics. Multiple trials have examined manual handling training—teaching people to squat instead of stoop, to protect their backs, and to use “proper” technique.
The result has been consistent: it does not reduce the incidence of low back pain or injury.
That doesn’t mean posture is irrelevant.
It means posture alone isn’t protective, as we were taught to believe.
Biomechanical studies also complicate the story.
Yes, different lifting strategies change how forces are distributed—between the spine, hips, and knees.
But spinal loading during stoop vs squat lifting is often similar, not dramatically lower with knee-dominant lifts.
And importantly: loading is not injury.
The spine is a load-bearing structure designed to bend, extend, rotate, and tolerate force. What it does not tolerate well is being underloaded for decades, then suddenly being asked to perform.
The same issue exists with deadlifts.
Despite how strongly people argue about “proper deadlift technique,” there are no RCTs proving that one deadlift style or one “correct” spinal posture reduces injury risk in isolation.
What is associated with lower injury risk?
– Gradual exposure
– Appropriate loading
– Consistency
– Supervision for beginners
– Building tissue capacity over time
Not rigid rules about spinal position.
This is the key point that often gets lost:
Fear-based movement advice doesn’t make people safer.
It makes them avoidant.
And avoidance leads to deconditioning—of muscles, connective tissue, bone, and yes, the spine itself.
That lack of durability or resilience causes harm... because now they're fragile. And now they'e at higher risk of injury.
So when I say that message “ruined a generation,” I’m talking about what happened downstream:
– People afraid to bend
– People afraid to lift groceries
– People who believe one wrong move will “blow out” their back
– People who never trained spinal tolerance at all
Now we’re at risk of repeating the same mistake—just with more jargon.
Good coaching isn’t “never bend your back.”
Good coaching is teaching people how to bend in various conditons, under appropriate load, with progression, so tissues adapt.
That applies to knees, hips, spines, shoulders—everything.
Technique matters, but capacity matters more. And capacity is built through exposure, not avoidance.
That’s why I posted what I did.
Not to dismiss form.
But to challenge fear.
Painful conditions like osteoarthritis share common risk factors with many co-morbidities across all of the bodily systems. We need to move beyond seeing pain as a "joint" or "muscle" or "bone" problem and see it for what it is...a systems problem.
frontiersin.org/journals/endoc…
Spinal cord stimulation patterns of care, re‐interventions, and costs for private health insurers, Australia, 2011–22: a retrospective observational study - Jones - Medical Journal of Australia - Wiley Online Library onlinelibrary.wiley.com/doi/10.5694/mj…
Why do Achilles tendons rupture during submaximal step-backs? 🤔
In my latest video, I break down cases like Jayson Tatum & Guy Sebastian—and the role of tendon fluid dynamics
Plus, stay tuned for a series on post-rupture elongation
youtube.com/watch?v=vGiNkR…
A randomized controlled trial of stem cell injection for tendon tear
nature.com/articles/s4159…
Stem cell injection into supraspinatus partial tears in patients with shoulder pain lasting more than 3 months was not more effective than control injections.
Just out!! Why do patients come for one visit then never show up again? We studied it-there are five reasons. Free access for 50 days here: sciencedirect.com/science/articl…
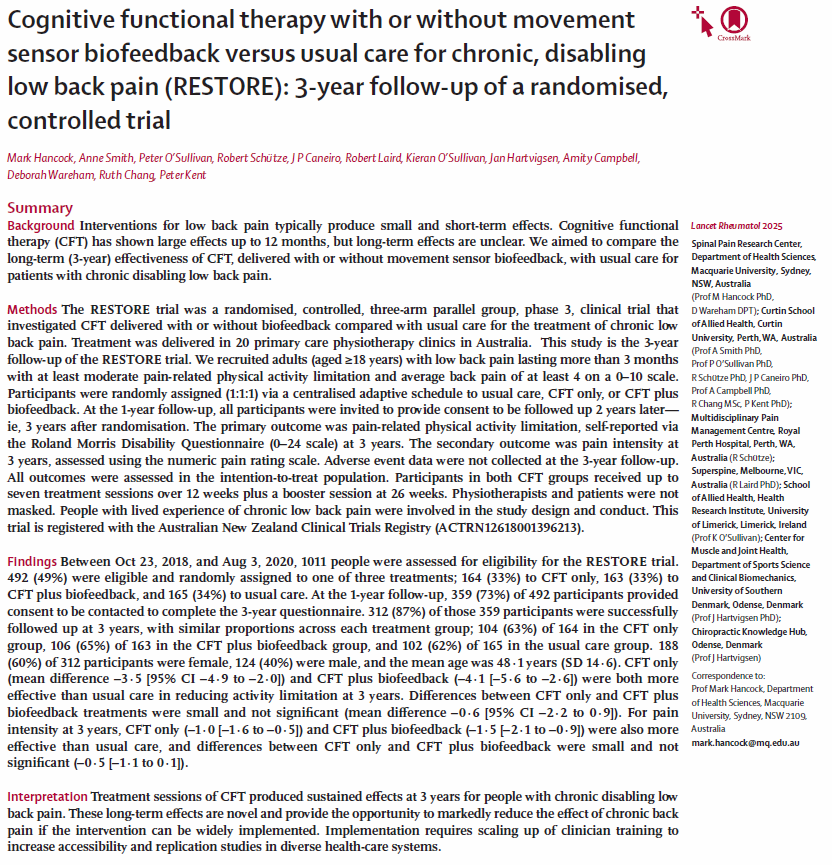
A new addition to the BMJ Rapid Recommendations series recommends against spine injections for chronic back pain.
“This will not be the last word, but it adds to a growing sense that chronic pain management needs a major rethink," says this Editorial bmj.com/content/388/bm…
There is a growing evidence-practice gap in the MSK pain field - termed a "super winked crisis". Most PT & DC curriculums & practitioners are slow to de-implement evidence-discordant or low-value MSK approaches.
Clinical benefit of physical rehabilitation after total hip and knee arthroplasty: A pragmatic, randomized, controlled trial (The DRAW1 trial)
pubmed.ncbi.nlm.nih.gov/39507936/
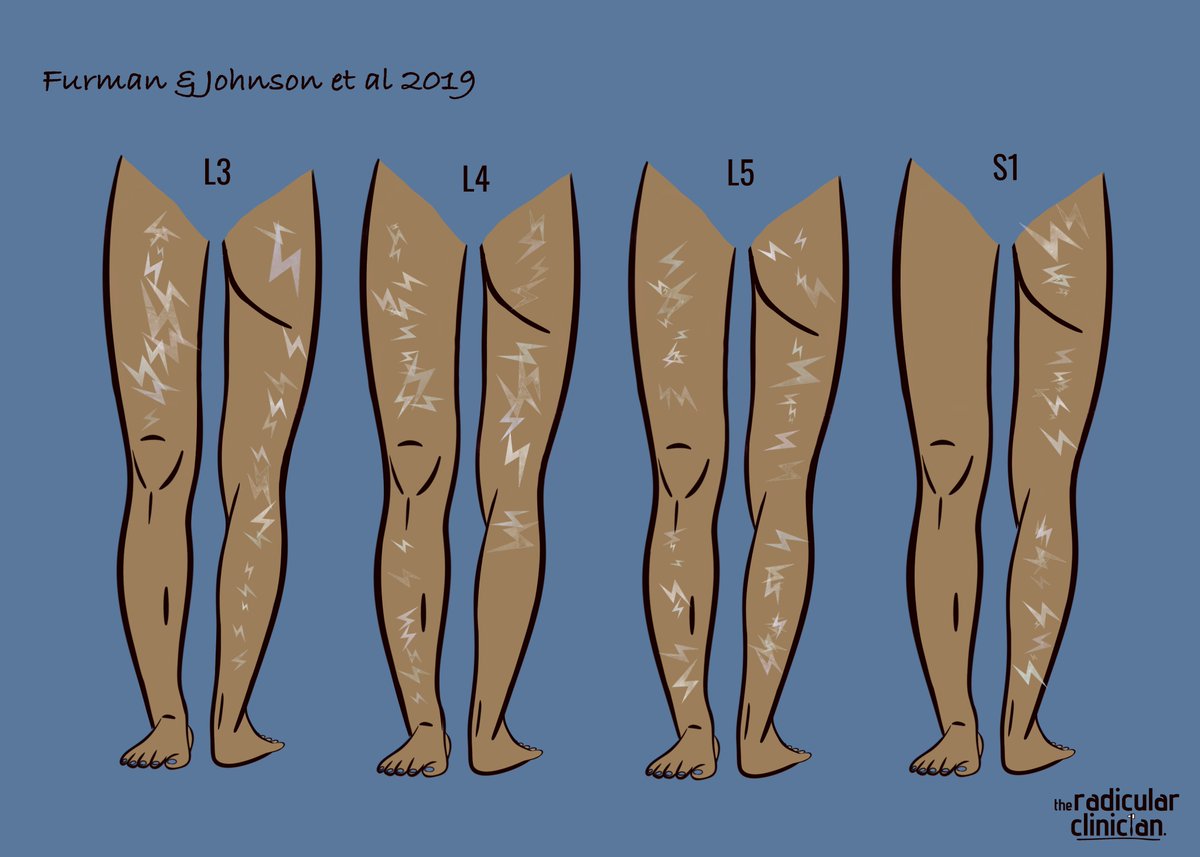
Lumbar radicular symptom referral patterns are variable and often do not conform to textbook dermatomal maps.
Here
Furman & Johnson 2019
Induced lumbosacral radicular symptom referral patterns: a descriptive study - ScienceDirect
sciencedirect.com/science/articl…
And here.
Hasvik et al 2022
Symptom descriptors and patterns in lumbar radicular pain caused by disc herniation: a 1- year longitudinal cohort study
bmjopen.bmj.com/content/bmjope…
Less is known about upper lumbar radicular pain referral patterns but this little study suggests that L1 and L2 much are likely to reside in the upper anterior leg.
sciencedirect.com/science/articl…
Ive certainly encountered a few cases of severe, isolated groin pain cases associated with L1 and L2 NRC. Worth considering as an uncommon differential.