Sabitlenmiş Tweet

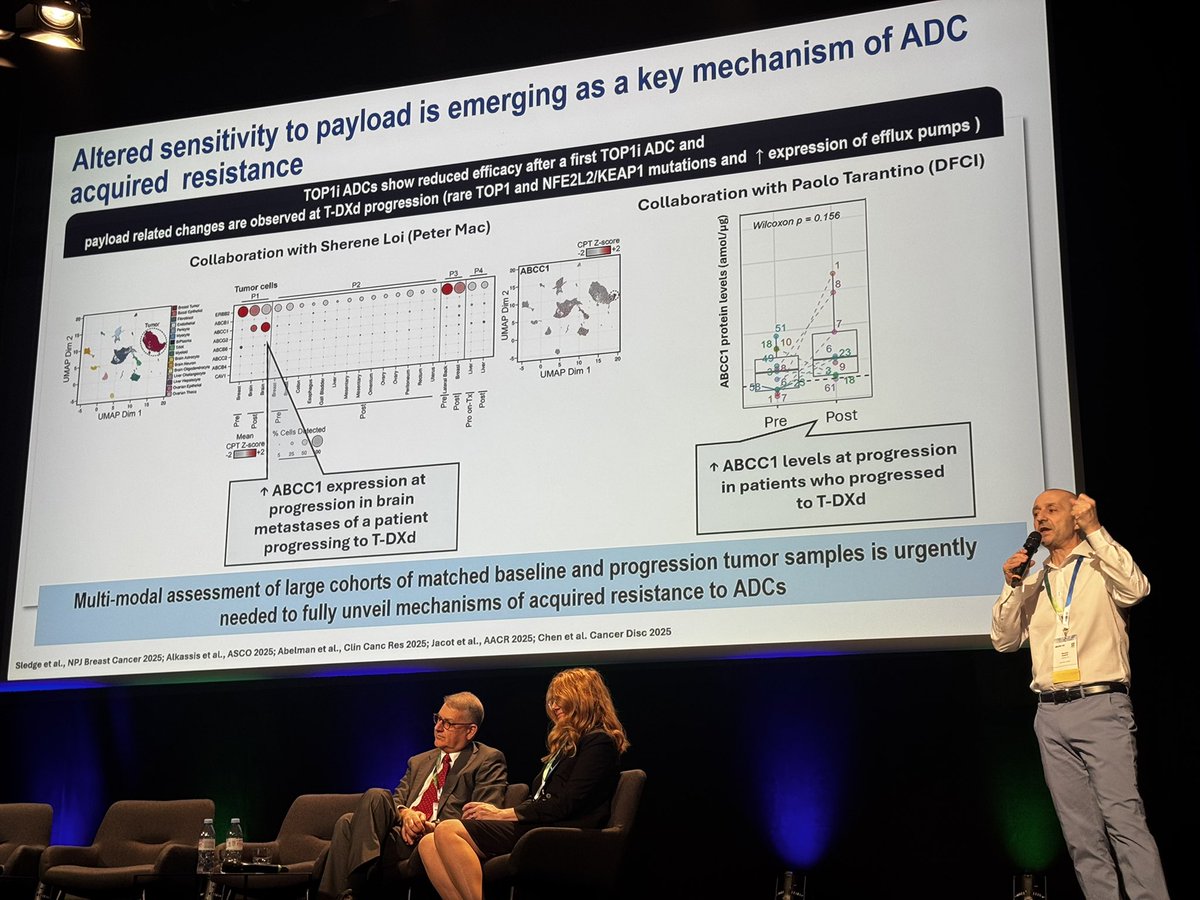
Out now in @ClinCancerRes: targeting the AHR pathway to overcome intratumoral immune resistance in bladder cancer tinyurl.com/39td758b
🚨We shouldn't give up on I/O in the treatment refractory setting in metastatic UC.
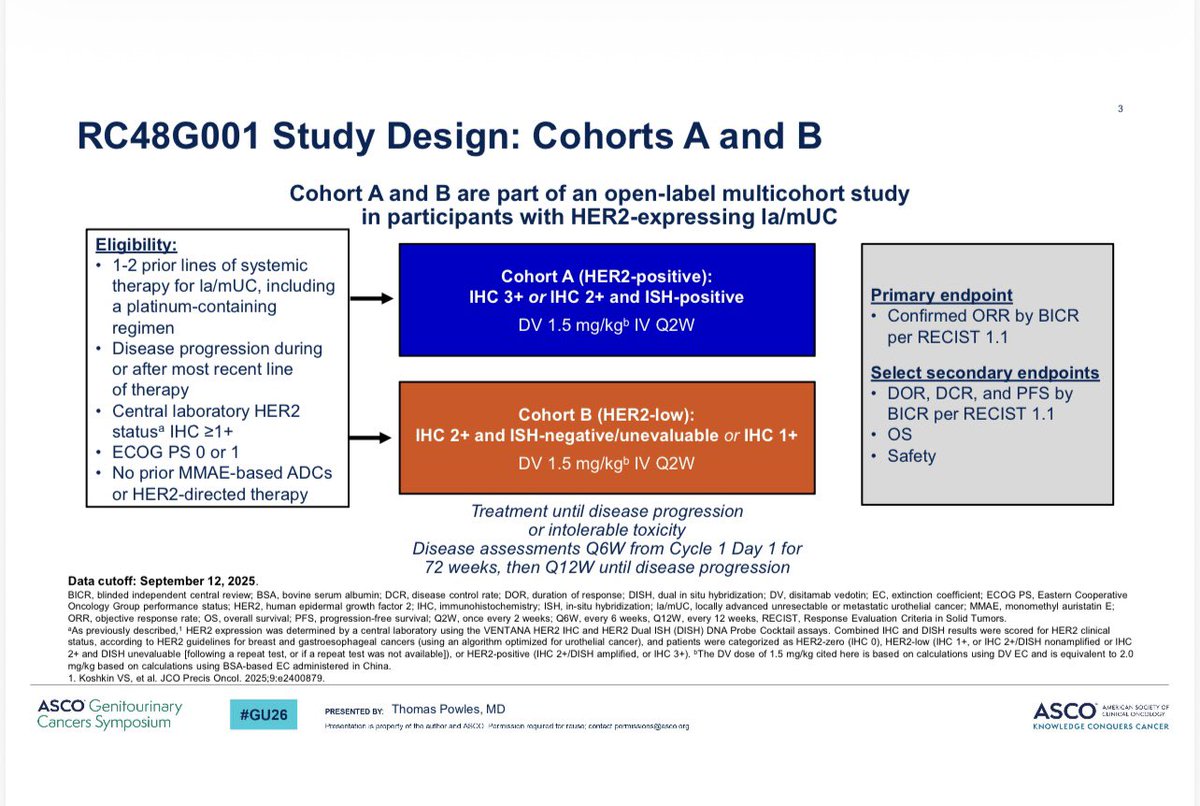
As EV/P and DV ± T move earlier in metastatic UC, later-line sequencing is the new challenge — overlapping toxicities (neuropathy, cytopenias, rash) often limit “what’s next?”
Tremendous effort from
@MeredithMcKean
@JCensits
@OAlhalabiMD
@abowmanmd
@alantanmd
@jasonlukemd
A tweetorial 1/6
English