Jackson Blythe retweetledi
Jackson Blythe
592 posts


Jackson Blythe
@drjacksonblythe
there be bad vibes in these waters
Kamilaroi country Katılım Ekim 2019
135 Takip Edilen87 Takipçiler

@DoverMarian @QLDCountryGP @healthgovau Some of the advanced skills in stream 2 are pretty nebulous. Like Indigenous health and remote med ASTs are project-based, AIM and paeds are basically just a year of reg'ing. All of those are fundamentally GP things that don't really change the level of service you provide...

English

@QLDCountryGP @healthgovau I do agree with you. Primary Care is the backbone of rural generalism too and Qld has clearly got an issue with this.
But at the same time, if you are working as a GP in hours only, not providing round the clock emergency care, the incentives should be adjusted for this.
English
Received this from @healthgovau today.
At least they're being honest about what they think of 'just' rural GPs.
If you're not a 'rural generalist' the Gov clearly considers you a lesser doctor in need of upskilling.

English
Oh, to be a lab
Sitting in the rain
Having recently discovered that you do,
in fact,
like water.

English
@QLDCountryGP @RACGPPresident I for one enjoy your void screaming and have found it most helpful as a void screamer in training, please continue
English
@drjacksonblythe @RACGPPresident The only reason any community needs an 'urgent care clinic' is because we don't have enough 'just' GPs due to government policy.
On current trajectory they'll chase their tail for the next decade while hemorrhaging money and still get nowhere.
I'll continue my void screaming.
English

Attention rural and remote GPs, the Rural Advanced Skills incentive applications are now open to recognise investment in specialist qualifications and credentialed skills. These are attributes that are so important for GPs working in the bush. #RuralGP health.gov.au/our-work/workf…
English
@john__qld Someone on here (might've been you?) labelled Katter ideology "agrarian socialism with senile characteristics" which is some of the funniest shit of all time
English
@QLDCountryGP @RACGPPresident Look, incentivising whole-of-community care across the acuity spectrum is simply not on the table. Have you considered opening an urgent care clinic?
English
@RACGPPresident This is good.
BUT
Once again the rural GP who does a bit extra in multiple areas (psychological counselling, advanced skin cancer excisions, ad-hoc local ED shifts, rural hospital admissions, on call for RACFs etc. misses out.
But pick one niche and get rewarded hey?
English
@PaulNWilliamz All part of the throwback noir aesthetic, I reckon
English
Jackson Blythe retweetledi

Someone needs to do an RCT on standard of care (SSRI+psychotherapy) vs a massive Samoan guy calling you 'big fella'.
English
Jackson Blythe retweetledi

Jackson Blythe retweetledi
@JudkinsSimon It's the false economy that rural health systems run on. 'Save money' by eroding pay and conditions = fail to attract permanent staff = fork out more for locums of variable quality, that come and go without any vested interest in the community.
English
@profmikegleeson Dislike. Photo is too busy with a tenuous link to content. Fonts are mismatched. The title looks vertically stretched and the thin text outline on the title is very 1998.
English

Here is a draft cover for our 4th edition Sport Nutrition textbook (Jeukendrup & Gleeson) which will be published in spring/summer 2024. We would like to know if (a) you like the cover or (b) you do not like the cover. Please reply to my message with a 'Like' or 'Dislike'. Thanks

English
@PaulNWilliamz Yes that must be a nightmare. There are obviously rules about when the government will subsidise but even on a private script a low-dose ICS/LABA inhaler at a chain pharmacy is $19 (=US$12.50) so the biggest barrier for me has been talking patients into changing meds around lol
English


@PaulNWilliamz Asthma is generally very poorly-treated in the community here (Australia). I almost never see PRN ICS/SABA and uncommon to even see regular ICS. Vast majority on SABA monotherapy and often taking like 6-8 puffs a day thinking this is ok. Doctor and patient factors at play I think
English
Jackson Blythe retweetledi
Ok what about this? You can choose a non-primary care specialty, but you have to spend 1 year in minimum security prison first. You want to be a dermatologist? 1 year in jail. Family medicine? Please proceed enjoy your freedom
Difficult problems require outside the box solutions
English


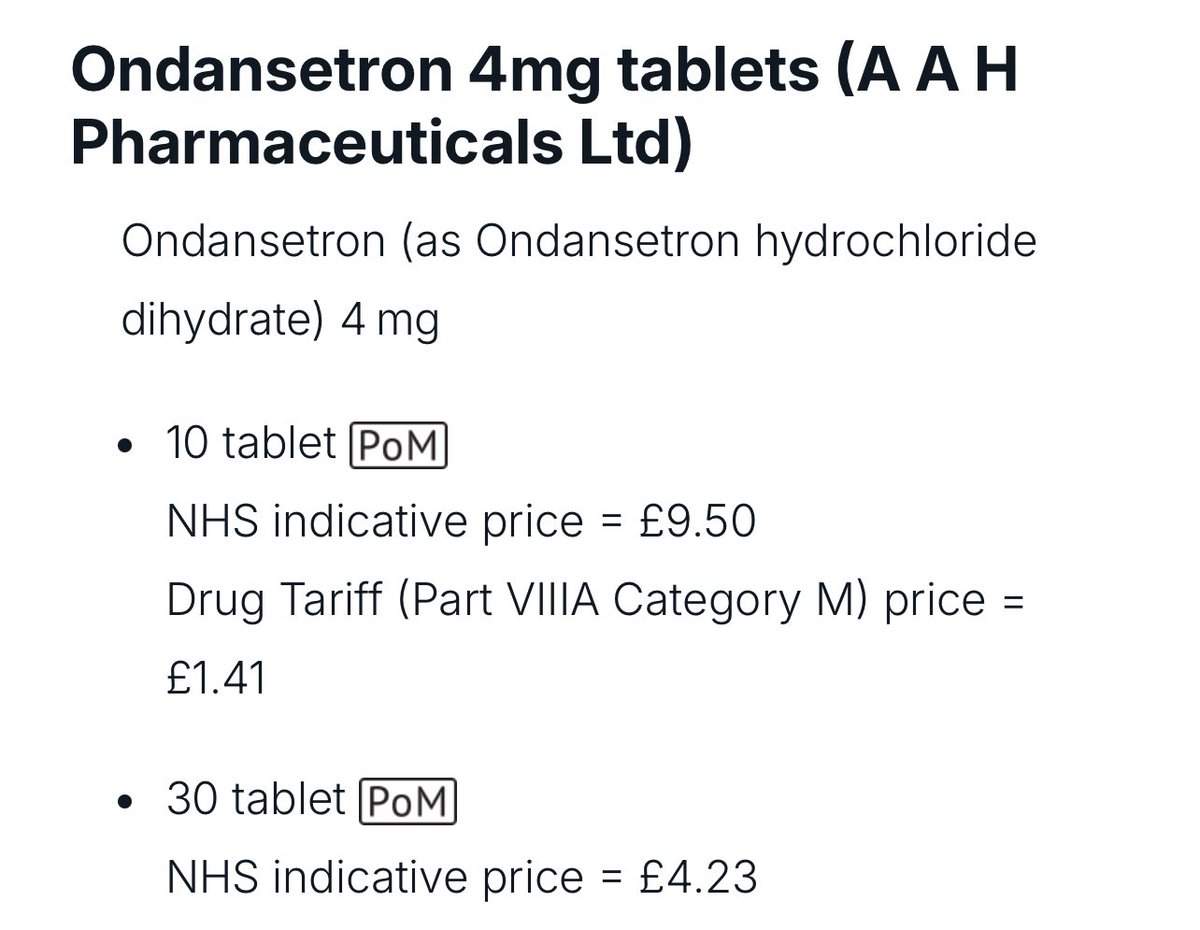
Ondansetron is a fantastic but underused treatment for diarrhoea predominant IBS ⭐️💡
English
@gronk_gronk Mine placed me in Adelaide so I think I might just walk into the ocean
English
@DoverMarian @ACRRM @RuralDoctorsAus @yourAMSA I am aware it's optional, and will be a great option for many as I said. But the advocates of this model never talk about the downside. I'm just saying people should be given all the info including the pros and cons of both, not just the benefits of SEM.
English
@drjacksonblythe @ACRRM @RuralDoctorsAus @yourAMSA It’s completely optional, Dr Blythe. If you’re a confident MBS biller, the SEM may not suit. I think Medicare turns people off and the SEM could be the “soft landing” people need to give it a try.
English
Attn Med students and Doctors in Australia,
Would the Single Employer Model (seamless continuation of leave entitlements from hospital, paid parental leave, a salary without Medicare fee-for-service) make GP training more attractive to you?
@ACRRM @RuralDoctorsAus @yourAMSA
English