Parth retweetledi

You are about to give parenteral B12. Which electrolyte must be checked first and what complication are you trying to prevent?

English
Parth
1.5K posts

@flozinatorMD
PGY 5 | Internal Medicine (AIIMS, New Delhi) | Alma mater (GMC, Rajkot)



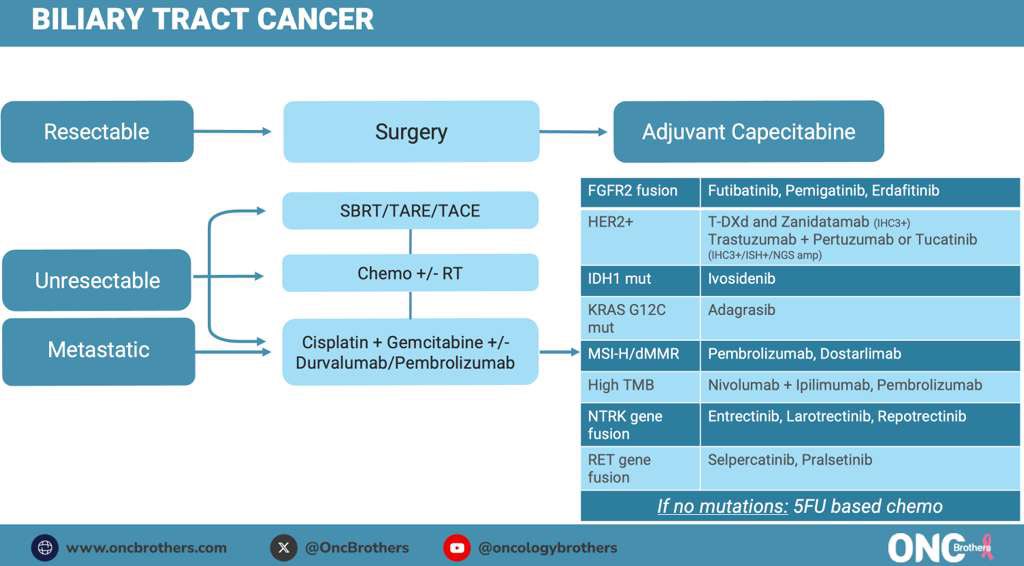
Here is the link to our full discussion with @SKamath_MD on #BiliaryTractCancer Treatment Algorithm! #Oncology #Cancer @ClevelandClinic @OncUpdates #OncTwitter #MedX youtu.be/1t0iJx4utEM?si…











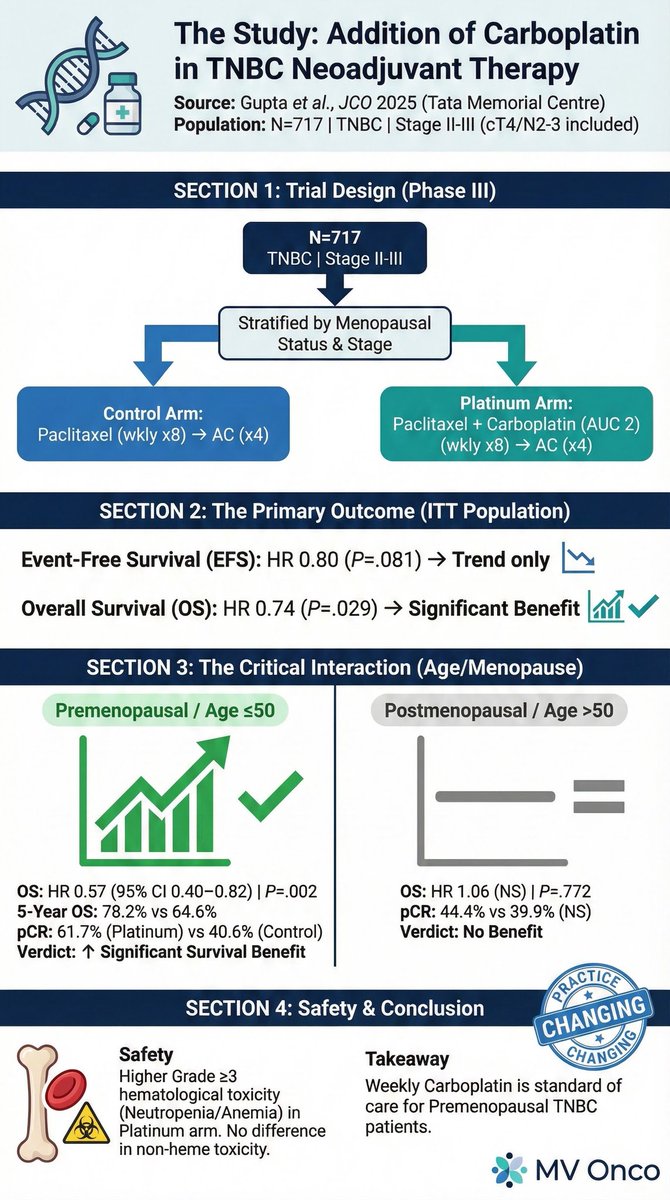




Triple Negative #BreastCancer highlights from #SABCS25 w/ @Dr_RShatsky: ✅ #RJBC1501 ✅ #CITRINE ✅ #TBCRC056 ✅ #OlympiaN Full Discussion: ⭐️ oncbrothers.com/sabcs25-tnbc ⭐️ Also on the “Oncology Brothers” podcast #OncTwitter #bcsm @OncUpdates