𝐏𝐨𝐬𝐭𝐞𝐫𝐢𝐨𝐫 𝐡𝐢𝐩 𝐩𝐚𝐢𝐧 𝐢𝐬 𝐭𝐡𝐞 𝐦𝐨𝐬𝐭 𝐨𝐯𝐞𝐫-𝐥𝐚𝐛𝐞𝐥𝐥𝐞𝐝, 𝐮𝐧𝐝𝐞𝐫-𝐫𝐞𝐚𝐬𝐨𝐧𝐞𝐝 𝐩𝐫𝐞𝐬𝐞𝐧𝐭𝐚𝐭𝐢𝐨𝐧 𝐢𝐧 𝐌𝐒𝐊 𝐩𝐫𝐚𝐜𝐭𝐢𝐜𝐞.
Conditions overlap. Referrals look identical. Patients arrive carrying labels that don't fit.
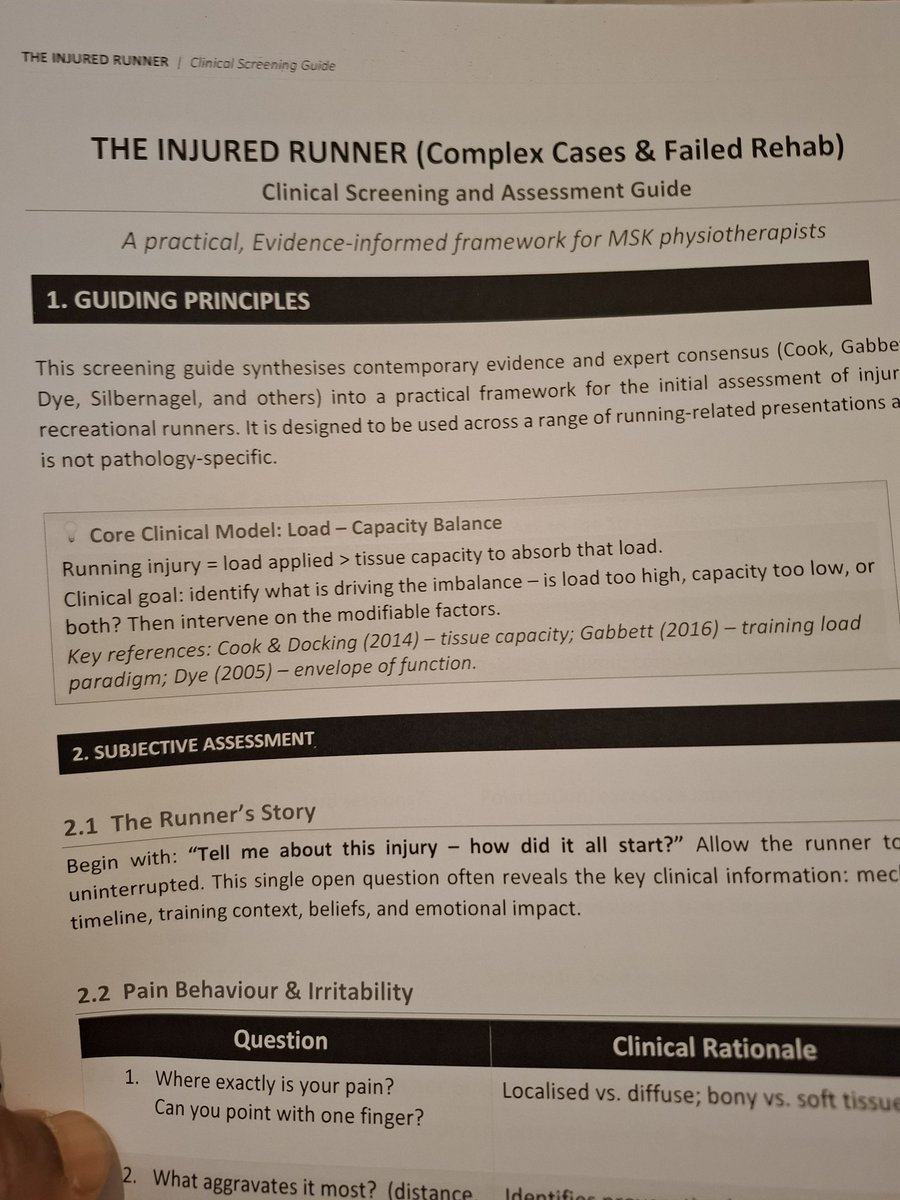
The fix isn't a longer differential list. It's a sharper reasoning sequence.
I've just published a clinical guide, walking through the framework I use in clinic and teach on my hip course:
→ Why labels fail
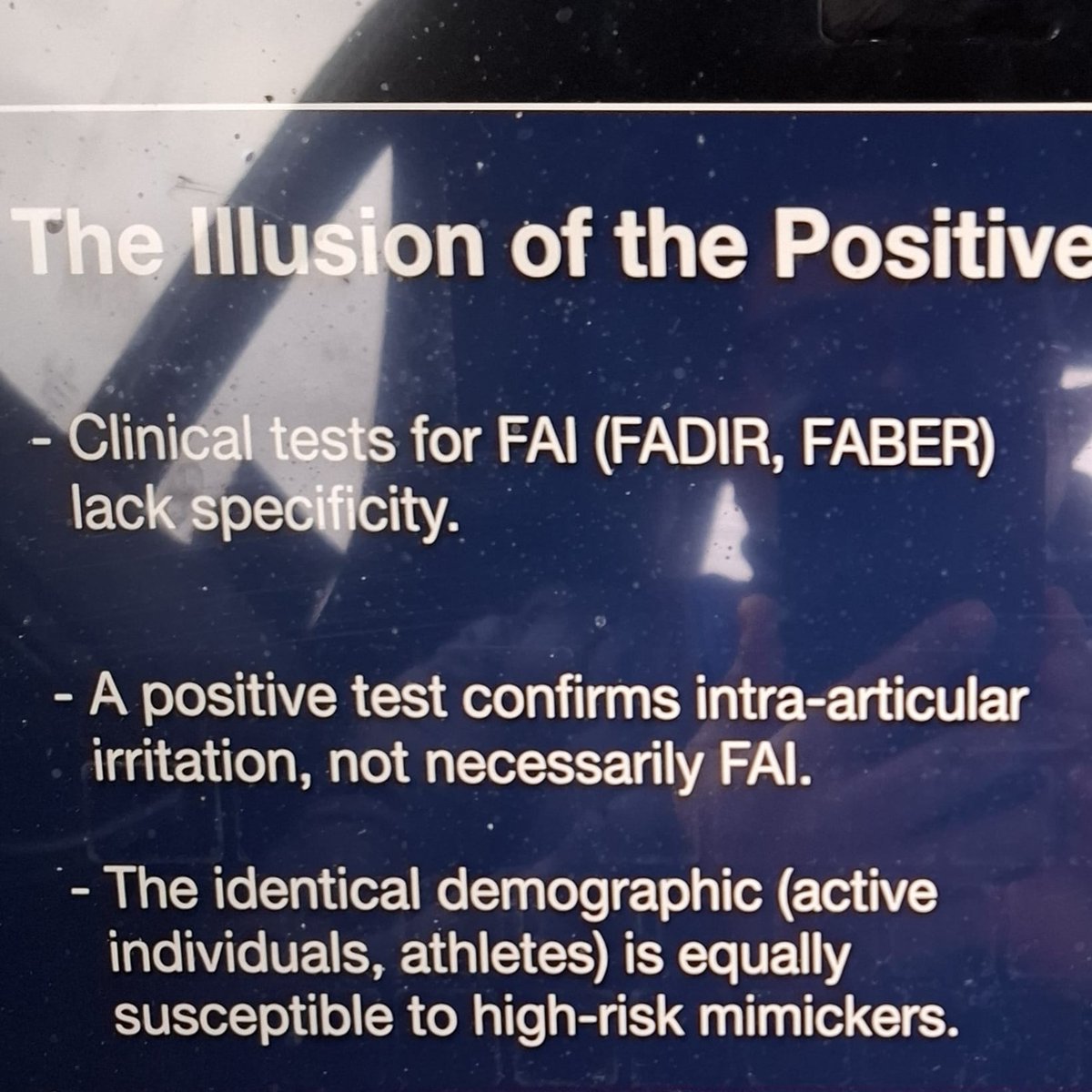
→ The 6 discriminating questions that narrow the field fast
→ The 3 clinical pathways that follow
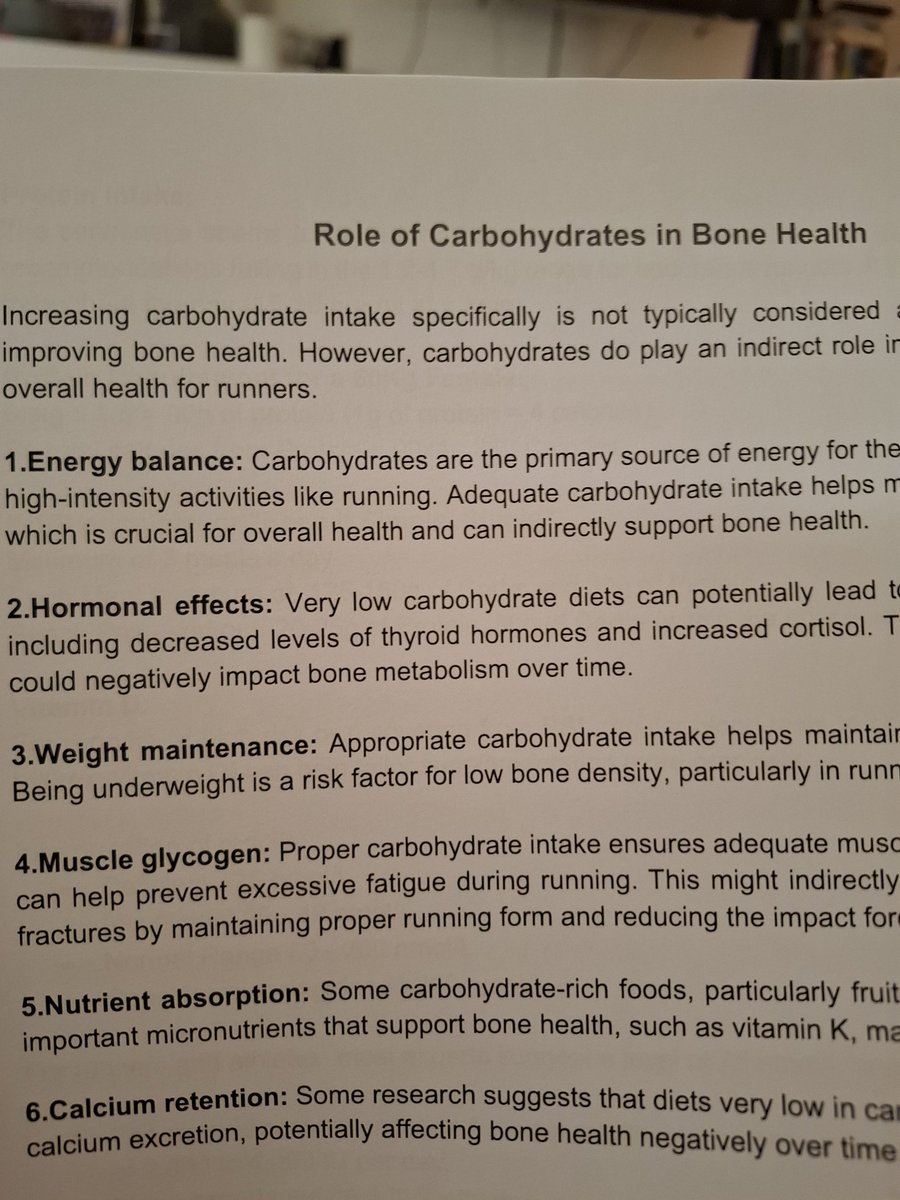
→ What commonly gets missed (Ischio-femoral impingement, pudendal entrapment, sacral BSI )
→ When to image and which modality answers which question
Free 14-page PDF guide inside it.
If it sharpens one assessment this week, it's done its job.
🔗 Link below to download
function-2-fitness.kit.com/0bd45c8f23
English