@RimaForAAPS Obviously, I think Rima is the best, but I may be a smidge biased. However, I can absolutely attest to her long-standing dedication to these issues. She's also a proven collaborator and team player. Perfect for this role.
I am excited to announce my candidacy for Ann Arbor Public Schools (AAPS) Board of Education.
I am running because I am passionate about addressing disparities, curriculum development & assessments, transparency, & diversity, equity & inclusion (#DEI ). #AnnArbor#A2SchoolBoard
@jpogue1 And as far as @jpogue1, can you imagine having access to THAT brain during a pandemic when rapid-fire critical, nuanced literature evaluation is absolutely essential? However highly you think of him, your bar is still way too low.
@jpogue1 We all know how intense/bewildering/exhausting/etc. it was to develop and maintain COVID guidelines for our institutions over the past year +; can you imagine NIH guidelines? Can't thank @IDPharmProf enough, who was there from the beginning and helped us all.
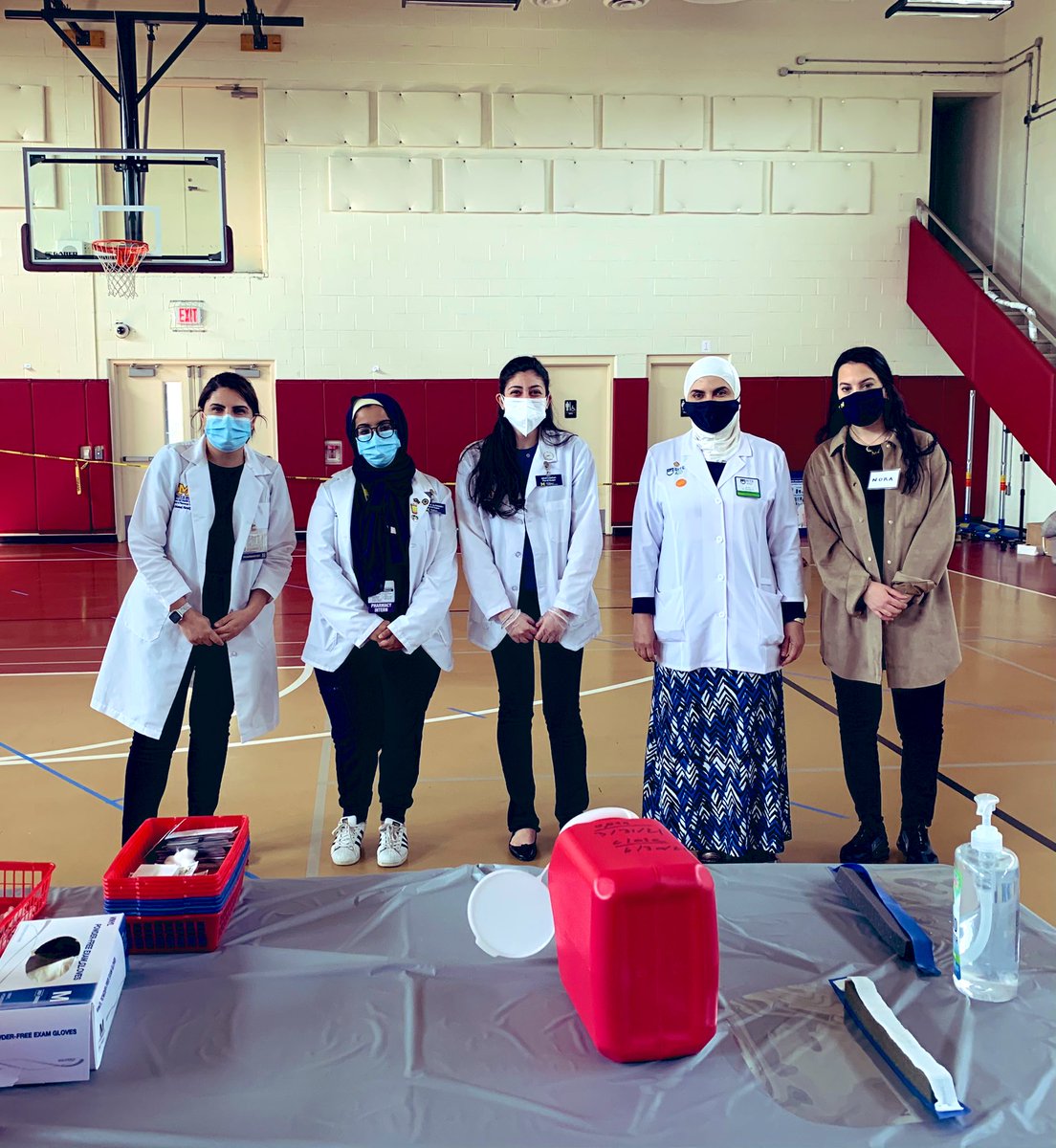
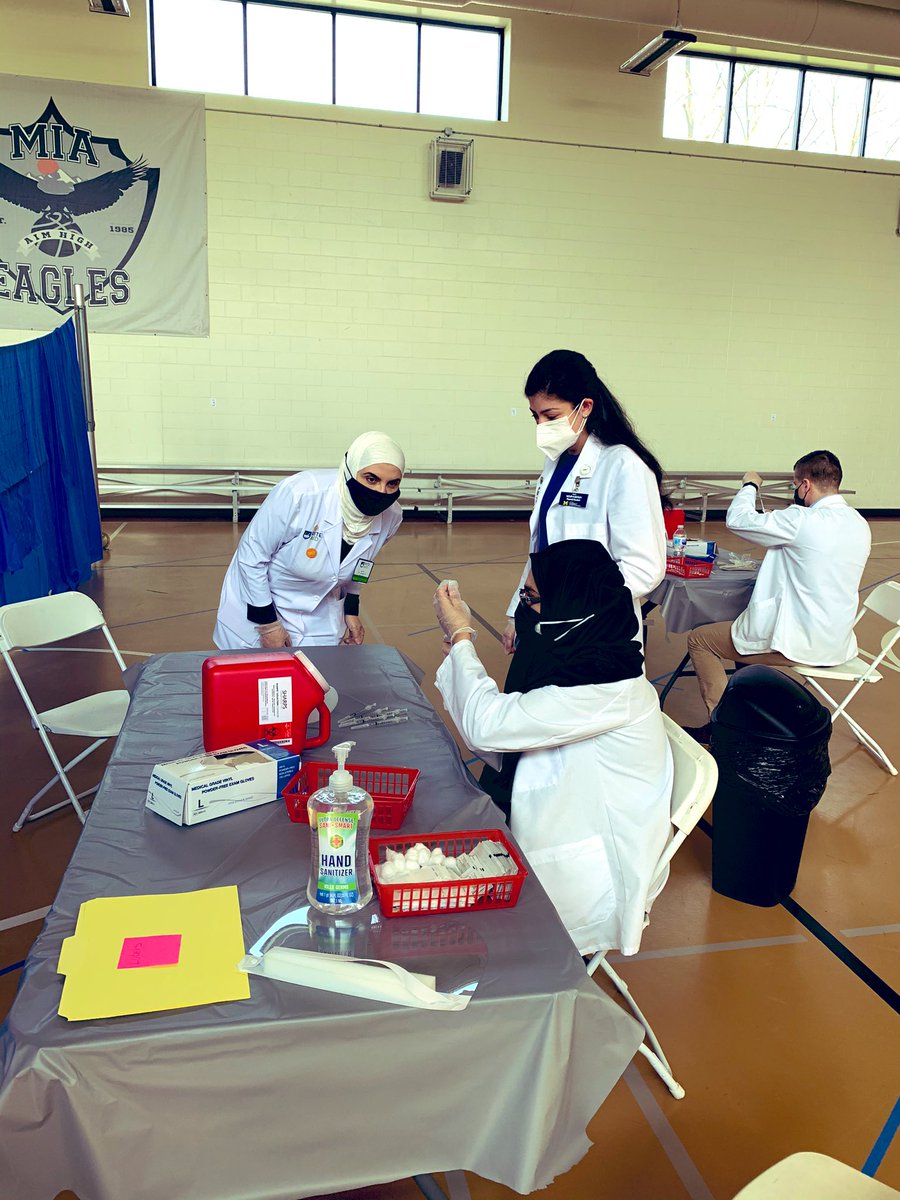
@RimaPharmD@UMichPharmacy@riteaid This team went from identifying vaccine that needed to be used by Monday on Saturday PM, to setting up this clinic, to vaccinating >125 members of the community within 24hrs. Astonishing.
Drs. @Tejal_N_Gandhi & @lindsay_petty discuss Michigan Medicine's Antimicrobial Stewardship Program #COVID19 guidelines & the streamlined process created to overcome significant barriers in delivering bamlanivimab to patients.
Pumped that we're reestablishing the @UICPharm to @UMichPharmacy pipeline with our current PGY1 Caleb Rux to be their PGY2 ID resident and current P4 and Wenzler research team member Michelle Lee for PGY1 🤗🤗
@ClancyNeil Agreed. But what is that patient population? I can't define it in anything approaching 'easy to use' (or at all). Even machine learning algorithm (for candidemia) could only hit 5% positivity (Bhavani Crit Care Med 2020).
@geschena But false positives don't get you in trouble if you are above a likelihood threshold where empiric treatment has value. This is the premise that needs to be tested and validated. The validation of the NPV part of the model is the easy part.
Interesting beta-D-glucan (BDG) study in high-risk ICU cohort for invasive candidiasis (IC), by group running EMPIRICUS MCF vs. placebo empiric Rx trial. Rigorous inclusion criteria, 11% IC incidence. Single BDG >80 when meeting criteria PPV/NPV 25%/95%. academic.oup.com/ofid/advance-a…
@ClancyNeil Right, but that's using a test to stop use that should have never started in the first place. Not arguing that's not real-life, but then the effort should be spent stopping 'fly by seat' use, not adding lab with lots of false positives that gets you into trouble.
@geschena I don't know how optimistic I am re: mortality, but only way an empiric/pre-emptive strategy will work is by getting to higher prevalence cohort than has been studied thus far. AF de-escalation will clearly work, if you are at a place that uses AFs on fly by seat of pants basis.
@ClancyNeil This is also informed by things like a.) MSG-01 algorithm is complicated but still misses half of IC cases b.) How much is SICU IAC outcome modified by (early) AFs? Most important time-sensitive intervention is source control, which also gets us cultures...
@ClancyNeil Agree re: NPV, but don't share your optimism about identifying a practical algorithm (+ BDG/T2) that improves outcome of ICU pts. Love to be proven wrong, but literature to date leaves me pessimistic.
@ClancyNeil I'd argue that RCTs that identified patients with that (5%-15%) threshold, and tested early antifungals, didn't show a pronounced benefit (Knitsch CID 2015; Schuster Ann Intern Med 2008; MSG-01).
@geschena Likely not, but other stratification strategies that get you within 5%-15% pre-test likelihood window should work, as well. Moreover, defining relatively high risk groups for IAC, rather than candidemia, is feasible.
@ClancyNeil But are EMPIRICUS 'high risk' criteria practical? Complicated rules don't work outside RCTs. From what I can tell it involves multi-site colonization assessment (mean 5 sites sampled at inclusion- eTable 1).
window where BDG actually makes empiric/pre-emptive AF therapy work. In EMPIRICUS, IC was dx'd in 14.7% (placebo) vs 8.5% (MCF) (p=0.14). If BDG was used to guide AF in this cohort, you go from 11% to 25% disease likelihood, which may be enough to get you above threshold for
Former @umichmedicine@UMichPharmacy PGY2 CritCare residents, RPDs, and faculty from ranging fron 2003-2021 in a peri-@SCCM Zoom meetup tonight - so great to see these folks!