Joel Mases retweetledi

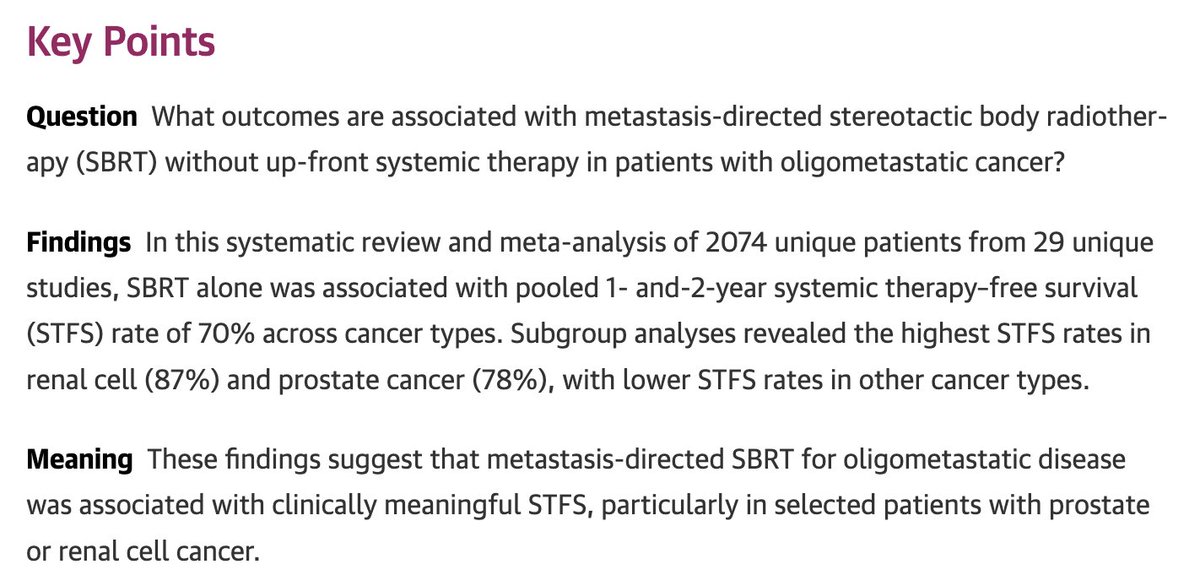
Let’s talk about prostate and urethra contouring on MRI. Three recent 📄📄📄 @SeibertLab
#radonc #ProstateCancer
🧵1️⃣
@IJROBP @RO_GreenJournal @ARRO_org @ASTRO_org @ESTRO_org

English
Joel Mases
2.7K posts


@joelmrbcn
Segarrenc de Guissona. Radiation Oncology MD. GU and hepatic cancer at @hospitalclinic. Views are my own. Barcelona



Have you ever wondered whether you need to hold systemic during RT due to concern for additive toxicity? See this 10 min video. Categorized by systemic type (cytoxic chemo, IO, TKI, BRAF, etc) & RT regimen (SBRT/conventional/palliative) Slides🧵& full video below. 1/8


I’ve really enjoyed this discussion and learning more about the topic. Sharing a reference sheet I put together a while ago comparing approvals across common disease sites. As an aside, Nanoknife appears to have somewhat unique approval language around “ablation of prostate tumors,” but still without a specific cancer treatment indication. Feedback welcome. bit.ly/FT_FDA_Approva…
@AndreaNecchi presents the final results of SUNRISE-2 with tar200+IO vs chemoRT showing no benefit of TAR200+IO compared chemoRT. Important negative study! @ASCO #GU26