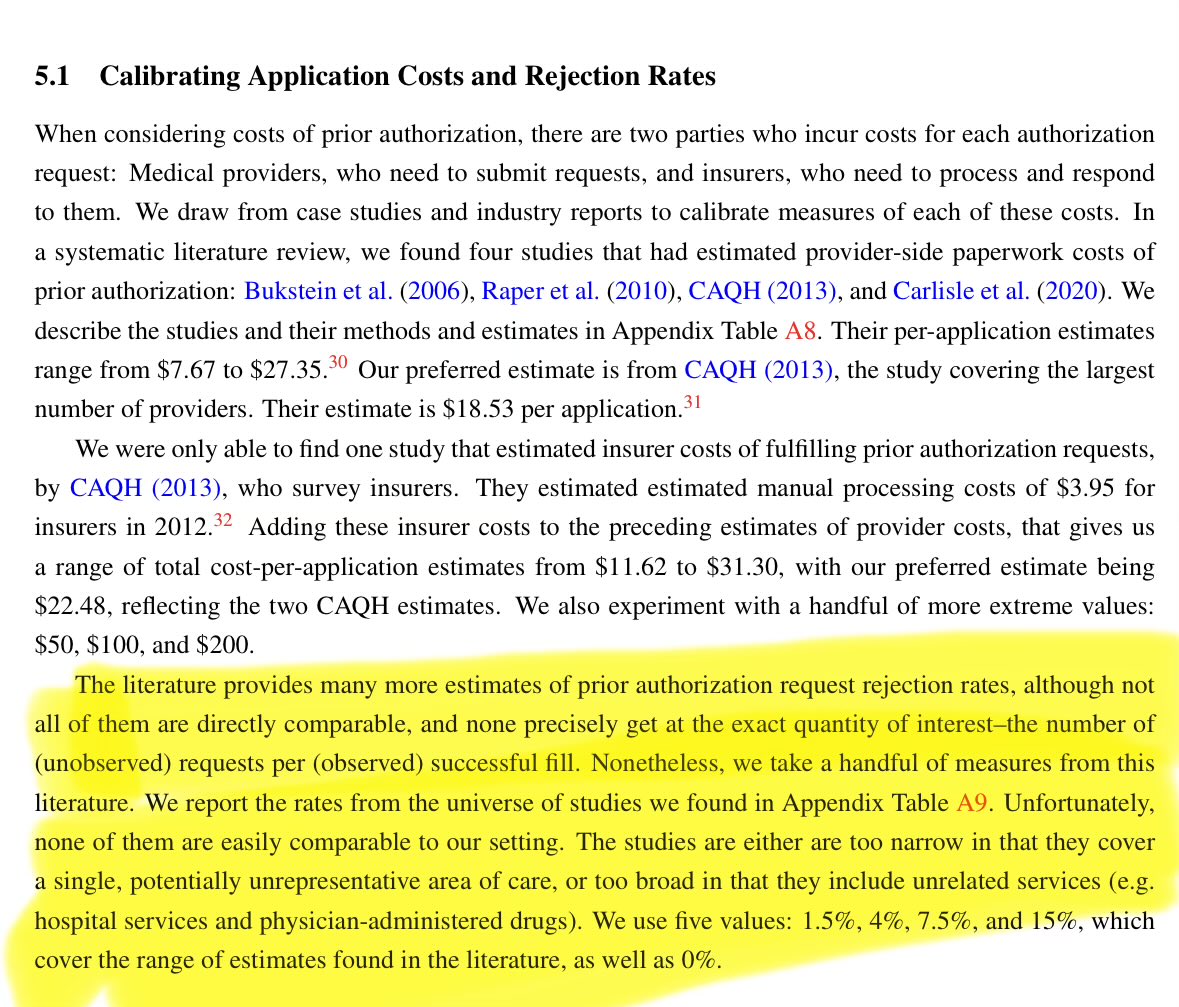
@zarekcb @ben_ippolito I missed the 0.299 restricted drugs per year for the average beneficiary so messed up my initial calculation in my initial skepticism
English
John Lin
156 posts
@johnlin08
Medical oncologist and health services researcher. Assistant professor, MD Anderson Cancer Center

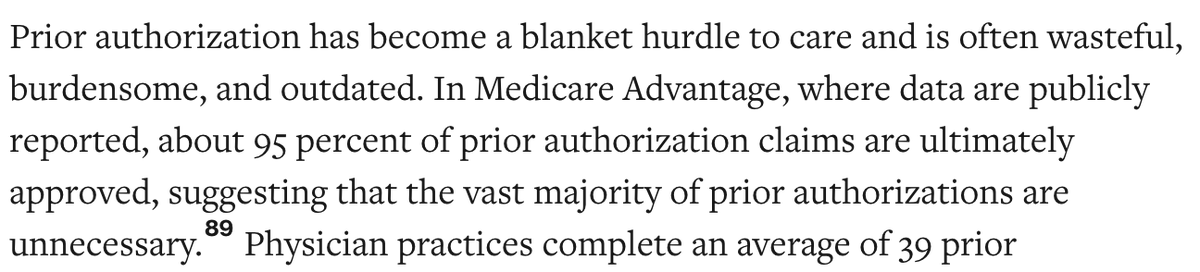


This is a stunning new statistic from @IQVIA_global: 70% of new prescriptions are initially rejected by private insurers. Many of those prescriptions are eventually approved, but it can take up to a year, and about one-quarter are still ultimately denied.