Sabitlenmiş Tweet

Rajan kanth
2.3K posts
@kanthMD
On a Journey..!!!







@mass_marion Cool. Cut all Medicaid CMS reimbursement rates by 50% and repeal the FMAP formula under Section 1905(b) that gives states lower per capita up to 66% more funding. (Of course we would see just about every rural hospital outside of the wealthy states fail in a manner of 6 months)



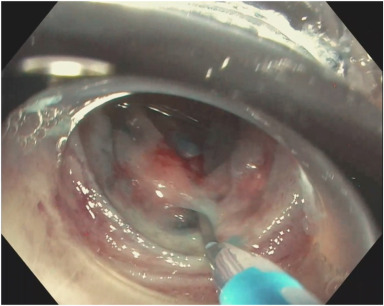
A typical endoscopic appearance of autoimmune atrophic gastritis, with an interesting finding of WGA. Learn how to recognize, assess, and approach gastric atrophy in a structured way at the Queen’s Optical Diagnosis Course 🗓 April 11–12, 2026 🔗 opticaldx.com