Sabitlenmiş Tweet
m.awan
5.8K posts



@AhmadRehanKhan Thank you for sharing.
Is home country residency required for this position?
English

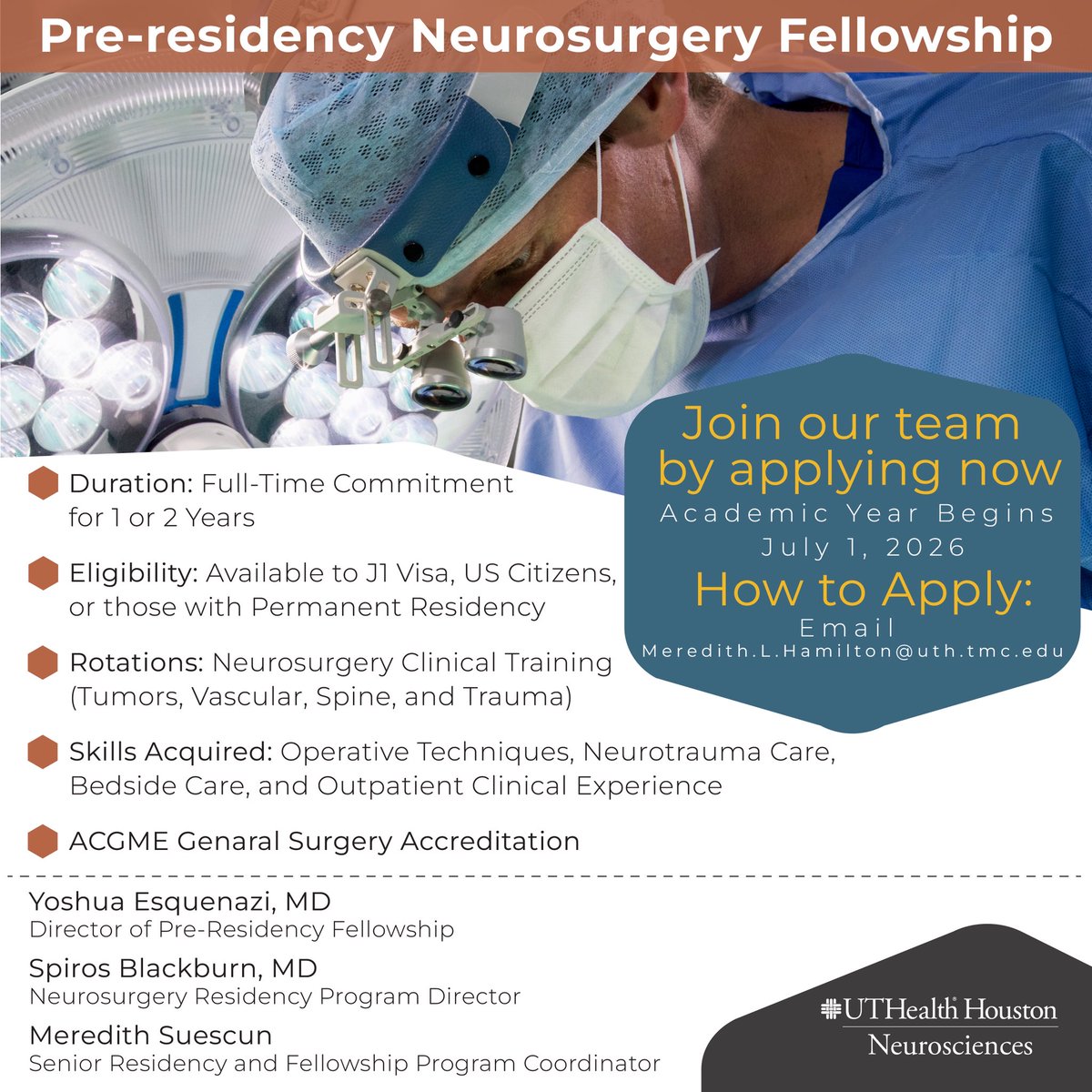
𝗡𝗲𝘂𝗿𝗼𝘀𝘂𝗿𝗴𝗲𝗿𝘆 𝗣𝗿𝗲-𝗥𝗲𝘀𝗶𝗱𝗲𝗻𝗰𝘆 𝗙𝗲𝗹𝗹𝗼𝘄𝘀𝗵𝗶𝗽:
Launch Your Neurosurgery Journey.
Step into the world of high-impact neurosurgery with the Pre-Residency Neurosurgery Fellowship at UTHealth Houston Neurosurgery
🗓️ Start Date: July 1, 2026
🧠 Real Exposure: Brain tumors, trauma, spine, and advanced neurosurgical care.
🚀 Designed to prepare you for residency and beyond
📩 Apply now: Meredith.L.Hamilton@uth.tmc.edu
Post courtesy of @NeurosurgUTH
Goshen, NY 🇺🇸 English
m.awan retweetledi

Your romantic partner is the single highest-dose pharmacological input in your daily environment. Bryan Johnson frames this as poetry. The data is more violent than that.
The Harvard Study of Adult Development tracked people for over 80 years. Relationship quality at age 50 predicted physical health at age 80 better than cholesterol, income, or career success. The mechanism is a specific neuroendocrine cascade. A supportive partner triggers oxytocin release, which suppresses cortisol, downregulates HPA axis activation, reduces systemic inflammation, and slows telomere attrition. Your cells literally divide longer before hitting senescence. The person sleeping next to you is either extending or compressing your biological clock at the chromosomal level, every single night.
Now run the numbers on the poison side. Married adults in one sample had a telomere T/S ratio of 1.70. Unmarried adults: 1.58. That gap held after controlling for diet, exercise, smoking, obesity, and social support. Divorced men in a Swedish cohort showed 46% higher relative mortality risk. A separate study of 3,526 adults found marital disruption was associated with shorter telomere length even after adjusting for neuroticism and lifetime traumatic events. The inflammatory profile of a high-conflict marriage looks nearly identical to the biomarker signature of chronic work stress or long-term caregiving burden.
This is the part people miss. Bryan said “somewhere between medicine and poison.” The pharmacology is more binary than that. Oxytocin from a quality partnership lowers blood pressure, reduces sympathetic nervous system activation, and improves immune surveillance. Chronic cortisol from a bad one drives the same oxidative damage to telomere cap structures that accelerates every major age-related disease. There is no neutral. The dose is always running.
A 2003 study found that more frequent partner hugs correlated directly with lower resting blood pressure and heart rate. The cardiovascular system responds to your primary attachment bond the way a tissue responds to a drug. Dose, frequency, duration.
“Medicine and poison” is the right frame. But Bryan undersold the dosage. This is the single largest uncontrolled variable in every longevity protocol on Earth, and almost nobody is tracking it.
Bryan Johnson@bryan_johnson
It’s obvious in retrospect, but wasn’t intuitively clear earlier in life: your primary life partnership is somewhere between medicine and poison. Kate is medicine. Her mind tickles me, touch soothes, and essence animates. No life decision more important than who you journey with
English
m.awan retweetledi

No, they didn’t take “residency spots from US medical students”. There are ~41,000 offered spots in the US training match, and ~30,000 MD plus DO graduates each year. Congrats to King Edward Medical school in PK. I know several graduates, and they are very well trained.
Mary Talley Bowden MD@MaryBowdenMD
150 medical students from a single school in Pakistan just took residency spots from US medical students.
English
m.awan retweetledi

ruet e hilal committee se guzaarish hai mere eid roster ke mutabiq eid ka chand announce kia jaye
Eesti
m.awan retweetledi


This journey was never easy, but today it feels worth every step. I’m overwhelmed with gratitude seeing this email—thankful to the Almighty a million times. #Match2026
#Match2026
English
m.awan retweetledi

Surgery resident @AaronGilani asked why people close the fascia of trocar sites with a figure-of-eight suture instead of a horizontal mattress.
Let us look at these briefly via one of my experiments.
(1/ )
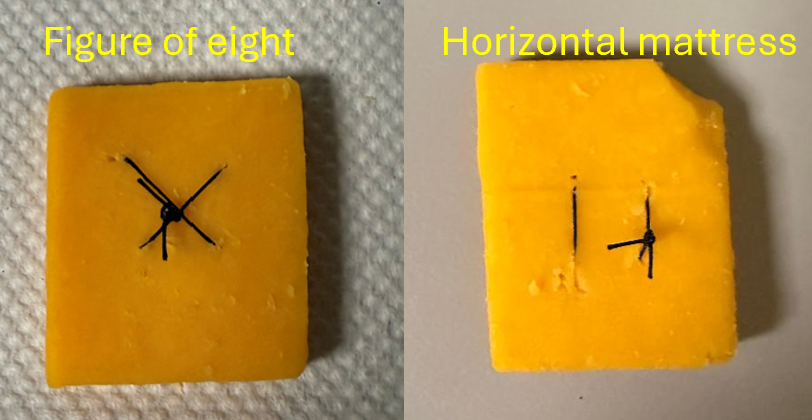
Aaron Gilani, MD, MBA@AaronGilani
I need @rbarbosa91 perspective on why everyone closes small facial sites with a single figure-of-eight, even though it’s a hemostatic suture pattern, as opposed to, for example, a horizontal mattress.
English
m.awan retweetledi
The largest real-world AI medical device trial just published. The results are... complicated.
The setup:
205 NHS primary care practices. 1.5 million patients. Eko Health's AI-enabled stethoscope vs. standard care.
Published in The Lancet (Feb 14, 2026). Nature Medicine dedicated a commentary.
This is how you test AI in healthcare. Not lab benchmarks. Real clinics. Real doctors. Real patients.
The headline finding:
When clinicians actually used the AI stethoscope, detection rates jumped:
• Heart failure: 2.3X
• Atrial fibrillation: 3.5X
• Valvular heart disease: 1.9X
The algorithm works. No question.
The problem:
The intention-to-treat analysis showed no significant difference between intervention and control groups.
Translation: on average, across all practices, patients weren't diagnosed any better.
Why?
Implementation gaps.
The AI stethoscope improved detection dramatically — when used. But adoption was inconsistent. Workflow integration failed. Some clinicians ignored the alerts. Some forgot the device. Some didn't trust it.
The algorithm was sound. The humans were the bottleneck.
The deeper lesson:
This is AI's dirty secret in healthcare. We obsess over model performance — AUC, sensitivity, specificity. But the real challenge isn't building the model. It's getting clinicians to use it.
An algorithm with 95% accuracy that sits in a drawer is worse than one with 80% accuracy that's actually deployed.
What the commentary said:
Nature Medicine called it "the perils of implementation gaps."
The gap between "works in theory" and "works in practice" is where most AI healthcare projects die.
My take:
This study is actually good news for AI in medicine. It proves the technology works. The detection improvements are real and substantial.
But it also proves that deployment is harder than development. UX matters. Workflow integration matters. Clinician trust matters.
The next generation of AI medical devices needs to be designed with implementation in mind, not just algorithmic performance.
We're entering the "implementation era" of AI healthcare. The low-hanging fruit of algorithm development is picked. The hard work now is making these tools actually useful in chaotic clinical environments.
TRICORDER is a roadmap for what to fix. Not a reason to stop.
Sources:
• thelancet.com/journals/lance…
• nature.com/articles/d4159…
• ekohealth.com/blogs/newsroom…
English
m.awan retweetledi

Anticoagulation therapy is the foundation of acute PE management. Use of DOACs and LMWH allow for rapid and predictable anticoagulation therapy in most patients with acute PE. Further management strategies are dictated by individual risk factors for adverse events. These include the measurement of biomarkers, RV size and function on imaging, and hemodynamics.
Informed by these risk factors, decisions can be made about the utility of advanced interventions, including catheter-directed thrombolysis, mechanical thrombectomy, surgical embolectomy, and extracorporeal membrane oxygenation. Use of a PERT to facilitate decision-making around acute interventions is recommended.
✍🏼 @GoldbergJBCTMD @Dkadiandodov @RosovskyRachel @sabeedak1 @hjcox_pvd @JunLiMD @mnyoung1

English
m.awan retweetledi

🚨 The 2026 AHA/ACC PE guidelines changed how we think about pulmonary embolism.
Not just new treatments — a new clinical framework.
Say goodbye to “massive vs submassive.”
Meet A–E PE Clinical Categories 🧵👇
English
m.awan retweetledi
There is nothing wrong with celebrating culture or having fun, but let’s be honest about what this has turned into.
Basant today is not what it once was. Over the years it has become inherently dangerous, no matter how many precautions are claimed. Sharp and lethal strings are still in use, and the risk of serious injury or death is real. I sincerely pray we do not witness tragedies again.
What hurts more is the misplaced prioritization. When over 4,000 doctors left Pakistan in 2025 and we continue to have one of the lowest literacy rates in South Asia, it is painful to see massive public funds spent on spectacles instead of strengthening education and healthcare.
No sane person is against Lahoris enjoying themselves. This is not about fun. It is about choices. And time and again, those in power have shown that the welfare of the poor, the middle class, and the educated is not their priority.
#BasantFestival #lahorebasant
#BasantReturnsInPunjab
Faizan@faizannriaz
People saying “they also celebrate festivals” are missing the point on purpose. Yes, they celebrate. No one denied that. The difference is festivals are a small part of their lives, not their main achievement. The rest of the year, they’re building companies, doing research, running factories, exporting products and competing globally. USA, Japan, UK, Australia didn’t give world Halloween or Bull festivals. They gave the world Apple, Google, Toyota, Microsoft, Samsung, SpaceX, Pfizer. They produce scientists, engineers, Nobel winners, CEOs and innovators. Their youth dreams about startups, labs and global careers. My phone isn’t made in Pakistan. My laptop isn’t. Most medicines aren’t. Most machinery isn’t. Even in 2026, we’re still importing basics. Meanwhile, we feel proud because we flew a piece of paper for a week. They enjoy festivals after building systems. We use festivals to escape reality. So yes, celebrate if you want. But don’t pretend this mindset leads to progress. Until we value skills, education, productivity and innovation more than temporary fun, nothing will change.
English
m.awan retweetledi

m.awan retweetledi


m.awan retweetledi
