@maddstone1 Yeah, the 819 kidney data looks really amazing. It appears to be rapid and durable. I am expecting a 80-90% CRR rate @ 6 months, which would be revolutionary for this disease.
@maddstone1@JessieChimni You are correct.
Strange strategy here. I assume at some point once safety and efficacy signals emerge using 839 that 819 will be phased out in these indications. One will need to cannibalize the other.
@maddstone1@JessieChimni No idea. Sell the news? They did shift SLE, IIM,AAV, SSc over to 839 (and added RA!). It looks like 819 will just be LN. Maybe that timeline slip is the cause.
@maddstone1@JessieChimni Yep, single arm, 53 patient target with CRR at 6 months as the primary endpoint. 15 month target timeline, though they stated that they have an internal goal of completing the trial in 12 months.
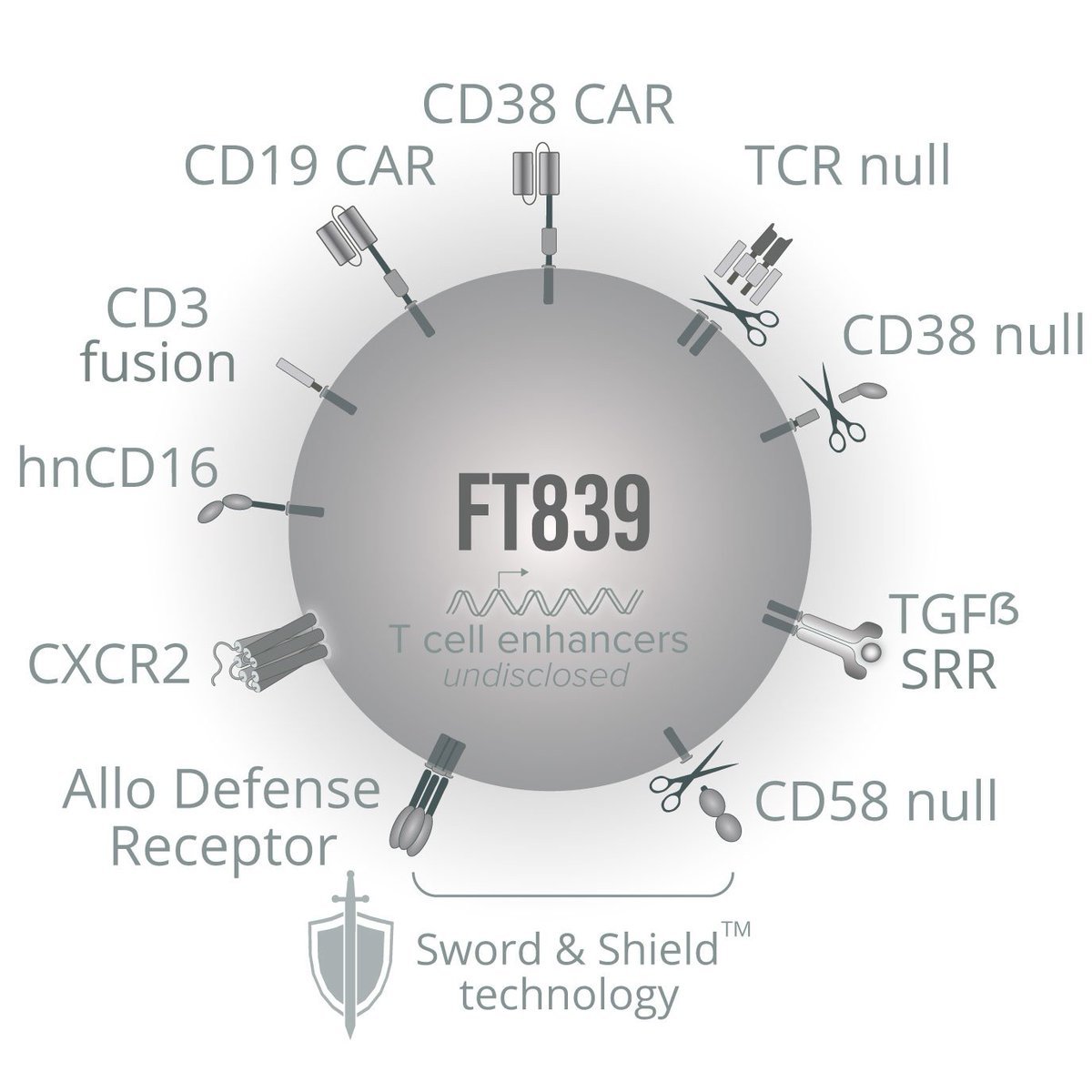
@AscendingBio $FATE I hope a significant part of the ASCO poster is the sword and shield cellular expansion kinetics (across 2 doses) and the persistence of the cells. Given stock price the assumption is that sword+shield won't work. However, the CRC patient response indicates otherwise!
$FATE CORRECTION:
UPDATE -ASGCT Poster Title & Abstract (May 11-15) - Preclinical Only
"CAR T cells Targeting pan-Tumor Antigens MICA/B can be Uniquely Combined with SOC Treatments without Conditioning Chemotherapy for Broad and Effective Therapeutic Application in Cancer"
The abstract was just published. This poster will focus on preclinical data.
There is still the presentation at ASCO (this is a poster, day and time TBA, abstract released May 21):
"Preliminary phase 1 results of a MICA/B-targeted CAR T cell designed to overcome solid tumor escape mechanisms and avoid the requirement for conditioning chemotherapy."
(So, this gets somewhat confusing because there are presentations at EULAR, ASGCT, and ASCO. In addition, there was a recent presentation at AACR. There has only been a press release from Fate for AACR. Some of us are digging and finding these presentations prior to Fate PR. There could be more that we have missed.)
distribution.us.m-anage.com/from.storage?i…
$FATE EULAR Oral Presentation Title
Off-the-Shelf Dual-CAR T-Cell Therapy: Targeting B and T Cells in Autoimmune Disease Without Preconditioning
Thursday, 4 June, 08:15 - 08:25 BST
@AscendingBio I guess that makes sense. Position it as "redosing available every 6 months" doesn't require them to prove years long durability.
I was pleased to here 12 month internal target for pivotal.
I did notice that comment. I think it is quite strategic. That framing takes you on the quickest path to FDA approval.
Yet, I will say that I do not expect many to need redosing. That is especially the case at the higher dose.
It is time to have a sense of urgency at getting a product to market. It is fine to work on improving the product especially working towards a no chemo treatment, but priority one is get that initial FDA approval!
$FATE Today's Conference
I always find myself listening intently for any new details about those receiving the cancer treatments.
We had previously been informed about a late stage colorectal cancer (CRC) patient. He is a 45-year-old male with seven prior lines of systemic therapy. Today, we learned that those prior treatments happened over 5 years with no meaningful reduction in disease burden.
We had been told that he was treated with 2 doses of FT836 at 300 million cells in the cetuximab combination arm without any conditioning chemotherapy. Today, we learned that treatment has continued at a higher dose (presumably 900 million cells).
Previously, we were told that his response to treatment included "a greater than 50% reduction in carcinoembryonic antigen (CEA) levels and significant reduction in lactate dehydrogenase (LDH) levels at Day 29 post treatment, with tumor reduction seen across all target lesions of approximately 20% decrease in the sum of diameters at the 46-day evaluation scan."
We are told to expect more cancer treatment results at ASCO: May 29 - Jun 02, 2026.
@AscendingBio $FATE - Listened to Leerink conference. At the very end mentioned plans for T1D. Immune depletion w/839, then implant allogenic islet cells. Belief is that during immune reconstitution these islet cells would now be recognized as "self". Totally amazing if this works....
If they can find a way to target the right cells, they have a chance of a cure. I read there are several different possible approaches. One way is to takeout the autoreactive CD4 and CD8 T cells that attack pancreatic β‑cells. I do not claim to fully understand the details.
I do not think Fate has put significant work into this yet, yet it caught my interest.
$FATE FT839 Indications
Interesting comments on this week's call about the potential to use FT839 in a variety of complex autoimmune diseases including Rheumatoid Arthritis and Type I Diabetes.
I may have the opportunity to speak to Bob Valemere, CEO of $FATE, over the next couple of weeks. Let me know if you have any questions regarding the trial and/or the business. Of course, I will be discussing publicly available information only.
@JessieChimni Can I get one more? This one might be more interesting and enlightening: "What is the most likely reason the iPSC platform could fail clinically?"
@JessieChimni My question: What specific clinical or regulatory milestone over the next 12 months are you most excited about and what probability would you assign to achieving it?
@JessieChimni@vksandhumd@FinanceKamal SRI-4 (vs SRI-6) as primary for a ~30-pt 819 pivotal is smart strategy.
SRI-4 has strong FDA precedent (Benlysta, Saphnelo) and maximizes statistical power in a small single-arm study. They can track SRI-6, SLEDAI=0, DORIS and highlight them! Lower risk, same upside.
I did not like that Bob mentioned SRI-4 as the primary endpoint he is discussing with the FDA. Made me wonder if he is seeing efficacy issues with 819; are they not achieving the the required immune re-set that auto CAR-Ts are achieving. Having said that, he mentioned that FDA considered it as a valid endpoint and other mABs had been approved with that endpoint. May be it is a strategic move to lower the bar for approval; assuming most patients achieve DORIS in the pivotal.
Anyone heard Bob's update on $FATE 819 at Leerlink? I will share my notes later this week. I did not come away with a great & positive feeling. Bob needs to present at more conferences to provide additional color @vksandhumd@FinanceKamal
@JessieChimni@vksandhumd@FinanceKamal 30/single arm is very bullish. Implies they are seeing 819 producing high, deep CRR rates with durability to justify such a small registrational dataset!
@JessieChimni@vksandhumd@FinanceKamal He is telling a lot. Why he picked Benda not CY, COG, 3rd gen for AIDs where T cells are drivers etc ... in 20 minutes. first 10 min intro was useless to me. I was hoping for something on 836/LDH
@ny1972_47 $FATE Very exciting result..and at the lowest dose! Late line CRC is probably the most challenging solid tumor setting. This result is prior to the "clinical response" assessment at Day 56. I think an official PR is very possible!
45 year old male who had received 7 prior lines of therapy, > 50% reduction in CEA levels and significant reduction in LDH levels at Day 29 post treatment, with tumor reduction seen across all target lesions of about 20% decrease in the sum of diameters at the 46-day eval scan.
$fate MSS CRC
IL-10-negative Tregs, on the other hand, suppress immune defenders — especially CD8+ T cells with strong anti-cancer capabilities. This subtype of Tregs is largely found within the tumor itself.
mskcc.org/news/msk-resea…