Sabitlenmiş Tweet
Moh'd Alhassan | محمد الحسن
88 posts

Moh'd Alhassan | محمد الحسن
@mohammedsa144
طبيب قلب Cardiologist
Katılım Ağustos 2021
131 Takip Edilen300 Takipçiler
Cardiology Note:
------------------
𝗛𝗼𝘄 𝘁𝗼 𝗱𝗶𝗮𝗴𝗻𝗼𝘀𝗲 𝗰𝗼𝗻𝗴𝗲𝗻𝗶𝘁𝗮𝗹 𝗹𝗼𝗻𝗴 𝗤𝗧 𝘀𝘆𝗻𝗱𝗿𝗼𝗺𝗲?
Any of these 4 criteria:
1) QTc using Bazett's formula ≥500 msec in the absence of a secondary cause for QT prolongation
2) QTc between 480-499 ms in repeated ECG in a patient with unexplained syncope in the absence of a secondary cause for QT prolongation
3) Presence of a definite pathogenic mutation in one of the LQTS genes
4) Schwartz risk score ≥3.5 in the absence of a secondary cause for QT prolongation
--------------------------------
Reference:
ACCSAP 2023

English
Cardiology Note:
-------------------
𝗔 𝗽𝗮𝘁𝗶𝗲𝗻𝘁 𝘄𝗶𝘁𝗵 𝗘𝗶𝘀𝗲𝗻𝗺𝗲𝗻𝗴𝗲𝗿 𝘀𝘆𝗻𝗱𝗿𝗼𝗺𝗲 𝗵𝗮𝘀 𝗼𝘅𝘆𝗴𝗲𝗻 𝘀𝗮𝘁𝘂𝗿𝗮𝘁𝗶𝗼𝗻 𝗼𝗳 𝟴𝟲% 𝗼𝗻 𝗿𝗼𝗼𝗺 𝗮𝗶𝗿. 𝗛𝗲 𝗶𝘀 𝗮𝘀𝘆𝗺𝗽𝘁𝗼𝗺𝗮𝘁𝗶𝗰. 𝗦𝗵𝗼𝘂𝗹𝗱 𝗵𝗲 𝗯𝗲 𝗴𝗶𝘃𝗲𝗻 𝘀𝘂𝗽𝗽𝗹𝗲𝗺𝗲𝗻𝘁𝗮𝗹 𝗼𝘅𝘆𝗴𝗲𝗻?
👇🏻👇🏻
"Supplemental oxygen is administered only as needed for symptom relief, but not to a target oxygen level.
Excess supplemental oxygen should be avoided as there is a potential risk of reducing the patient's hypoxia-mediated drive to ventilation"
"Studies showed that oxygen therapy has neither short- nor long-term beneficial effects"
-----------------------------
References:
- Uptodate website
-ahajournals.org/doi/10.1161/CI…
English
Cardiology Note:
-------------------
Systemic thrombolysis is not recommended for left ventricle (LV) thrombus due to the risk of embolization
------------------------
Reference:
ACCSAP 2022
English
Cardiology Note:
-------------------
A patient with history of AF on apixaban. He is scheduled for a cholecystectomy procedure. Should we bridge him with IV heparin during apixaban interruption?
👇🏻👇🏻
- Peri-operative bridging with heparin or LMWH in patients taking a NOAC has been linked to an increased risk of bleeding without any corresponding decrease in thromboembolic events.
- Consequently, when NOAC interruption is required for surgery, bridging is not recommended, except in a few high thrombotic risk circumstances (like patients with recent thromboembolic events within 3 months and patients who experienced a thromboembolic event during previous interruption of NOAC therapy.
- Post-operative DVT prophylaxis with LMWH should be considered in patients in whom NOAC therapy cannot be quickly restarted.
-------------------------------
Reference:
2022 ESC Guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery
#CardioTwitter
English
Cardiology Note:
-------------------
A patient underwent primary PCI after having anterior STEMI. CBC later showed a high WBC of 15,000
How do you interpret the high WBC in such a patient with STEMI, despite the absence of symptoms and signs of infection?
👇🏻👇🏻
"Elevation of the WBC usually develops within 2 hours after the onset of chest pain, reaches a peak 2 to 4 days after infarction, and returns to normal in 1 week; the peak leukocyte count generally ranges between 12 and 15 × 103/mL but occasionally rises to as high as 20 × 103/mL in patients with large STEMI"
"Experimental evidence suggests that the surge in catecholamines after coronary occlusion can mobilize leukocyte progenitors from bone marrow, thereby sustaining the inflammatory response following infarction"
--------------------------
Reference:
Braunwald's heart disease a textbook of cardiovascular medicine, 12th edition
#CardiologyNote
English
Cardiology Note:
-------------------
𝗜𝘁 𝗶𝘀 𝘄𝗲𝗹𝗹 𝗸𝗻𝗼𝘄𝗻 𝘁𝗵𝗮𝘁 𝗽𝗮𝘁𝗶𝗲𝗻𝘁𝘀 𝘄𝗵𝗼 𝗵𝗮𝘃𝗲 𝗺𝗼𝗱𝗲𝗿𝗮𝘁𝗲 𝘁𝗼 𝘀𝗲𝘃𝗲𝗿𝗲 𝗺𝗶𝘁𝗿𝗮𝗹 𝘀𝘁𝗲𝗻𝗼𝘀𝗶𝘀 𝗮𝗻𝗱 𝗔𝗙 𝗻𝗲𝗲𝗱 𝗼𝗿𝗮𝗹 𝗮𝗻𝘁𝗶𝗰𝗼𝗮𝗴𝘂𝗹𝗮𝘁𝗶𝗼𝗻 𝘁𝗼 𝗽𝗿𝗲𝘃𝗲𝗻𝘁 𝘀𝘁𝗿𝗼𝗸𝗲 𝗮𝗻𝗱 𝘁𝗵𝗿𝗼𝗺𝗯𝗼𝗲𝗺𝗯𝗼𝗹𝗶𝘀𝗺.
𝗦𝘂𝗽𝗽𝗼𝘀𝗲 𝗮 𝗽𝗮𝘁𝗶𝗲𝗻𝘁 𝗵𝗮𝘀 𝘀𝗲𝘃𝗲𝗿𝗲 𝗺𝗶𝘁𝗿𝗮𝗹 𝘀𝘁𝗲𝗻𝗼𝘀𝗶𝘀 𝗮𝗻𝗱 𝘀𝗶𝗻𝘂𝘀 𝗿𝗵𝘆𝘁𝗵𝗺 𝗼𝗻 𝗘𝗖𝗚, 𝘄𝗶𝘁𝗵𝗼𝘂𝘁 𝗮𝗻𝘆 𝗱𝗼𝗰𝘂𝗺𝗲𝗻𝘁𝗲𝗱 𝗔𝗙 𝗼𝗻 𝗘𝗖𝗚 𝗼𝗿 𝗛𝗼𝗹𝘁𝗲𝗿 𝗯𝗲𝗳𝗼𝗿𝗲. 𝗦𝗵𝗼𝘂𝗹𝗱 𝗵𝗲 𝘀𝘁𝗶𝗹𝗹 𝗯𝗲 𝗴𝗶𝘃𝗲𝗻 𝗮𝗻𝘁𝗶𝗰𝗼𝗮𝗴𝘂𝗹𝗮𝘁𝗶𝗼𝗻?
👇🏻👇🏻
"Patients in sinus rhythm, oral anticoagulation is indicated when there has been a history of systemic embolism or a thrombus is present in the LA"
"It should also be considered when transesophageal echocardiography shows dense spontaneous echocardiographic contrast or an enlarged LA (M-mode diameter >50 mm or LA volume >60 mL/m2)"
-----------------------------
Reference:
2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of ESC and EACTS
#CardiologyNote
English
@BinSeedi I do not how to solve this issue for you. It appears full text for others. Try a different browser or different mobile
English

@mohammedsa144 Out of no where, I’ve an issue with twitter, I can not see the full twit and just can see part of it with limitation. Do you have an answer to that please
English
Cardiology Note:
-------------------
Should you be worried to see an asymptomatic patient with a heart rate of 48 BPM several months after having bariatric surgery and ECG showing sinus bradycardia?
👇🏻👇🏻
- In a study conducted on patients who underwent bariatric surgery, 18% of them experienced asymptomatic sinus bradycardia.
- Heart rate ranged from 46 to 59 in those patients with bradycardia after surgery.
- Obese individuals have elevated levels of leptin which is released by adipocytes. After bariatric surgery, the concentration of leptin decreases, resulting in a lower heart rate.
- Sinus bradycardia is typically asymptomatic and does not necessitate treatment. Even in cases where it causes symptoms, it can be easily managed with parasymatholytics and does not require pacing.
-----------------------------
Reference:
Asymptomatic Sinus Bradycardia Following Bariatric Surgery
Malik, Manish G. et al.
American Journal of Cardiology, Volume 113, Issue 6, 1049 - 1053
#CardiologyNote
English
Cardiology Note:
-------------------
𝗣𝗼𝘀𝘁𝗲𝗿𝗶𝗼𝗿 𝗦𝗧𝗘𝗠𝗜
- Criteria to suspect Isolated posterior MI according to 2022 ACC:
1) Horizontal ST-segment depression in V1-V3
2) Dominant R-wave (R/S ratio >1) in V2
3) Upright T waves in anterior leads
4) Prominent and broad R-wave (>30 ms)
- Posterior infarction is confirmed by either the presence of ST elevation and Q waves in the posterior leads (V7-9) or new posterior regional wall motion abnormality on echo
----------------------
References:
- 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department
-Litfl website
#CardiologyNote

English
Cardiology Note:
-------------------
The USPSTF recommends that men aged 65 to 75 years who have ever smoked be screened for abdominal aortic aneurysm (AAA) with ultrasonography.
However, there are new updates in this subject.
According to the 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease, ultrasound screening for AAA is recommended/reasonable in both 𝗺𝗲𝗻 𝗮𝗻𝗱 𝘄𝗼𝗺𝗲𝗻 who are at least 65 years of age and have ever smoked, 𝗼𝗿 have first-degree relatives with AAA.
This updated guideline does not limit the age to less than 75 years, and it includes both men and women
---------------------------
Reference:
2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease
#CardiologyNote
#CardioTwitter
English
- US FDA has recommended evening administration for statins with shorter half-lives ( simvastatin < 5 hours).
- In contrast, the FDA suggests statins with longer half-lives to be administered in daytime (atorvastatin 14 hours, rosuvastatin 19 hours).
------------------------
Reference:
medscape.com/viewarticle/55…
English
Cardiology Note:
-------------------
𝗪𝗵𝘆 𝗶𝘀 𝗶𝘁 𝗿𝗲𝗰𝗼𝗺𝗺𝗲𝗻𝗱𝗲𝗱 𝘁𝗼 𝘁𝗮𝗸𝗲 𝘀𝗶𝗺𝘃𝗮𝘀𝘁𝗮𝘁𝗶𝗻 𝗮𝘁 𝗻𝗶𝗴𝗵𝘁 𝗶𝗻𝘀𝘁𝗲𝗮𝗱 𝗼𝗳 𝗺𝗼𝗿𝗻𝗶𝗻𝗴?
👇🏻👇🏻
- Most cholesterol synthesis occurs at night. Simvastatin has a short half-life, so if it is taken in the morning, its concentration will be minimal during the nighttime when most cholesterol synthesis occurs
- On the other hand, atorvastatin and rosuvastatin have longer half-lives compared to simvastatin. Therefore, it doesn't really matter what time you take them as they will still be present in high concentrations during the night, even if taken in the morning
------------------------
Reference:
- Wallace A, Chinn D, Rubin G. Taking simvastatin in the morning compared with in the evening: randomised controlled trial. BMJ. 2003 Oct 4;327(7418):788
#CardiologyNote
English
Cardiology Note
-------------------
Can we use amlodipine for patients with severe aortic valve stenosis and HOCM?
👇🏻👇🏻
When dealing with severe aortic stenosis, amlodipine should be used with caution since it can decrease coronary perfusion and lead to ischemia.
Similarly, caution should be exercised when using amlodipine in hypertrophic cardiomyopathy with LVOT obstruction, as reducing afterload may exacerbate the associated symptoms.
It is worth noting that according to Canadian labeling, amlodipine is contraindicated in severe AS and HCM with significant LVOT obstruction
-----------------------
Reference:
Uptodate website
#CardiologyNote
English
@abdulaziz_radhi ألف مبروك دكتورنا العزيز، ومن نجاح إلى آخر باذن الله
العربية

الحمد لله بنعمه تتم الصالحات
حفل التخرج ماجستير ادارة الاعمال
Graduation ceremony for Mater of Bussiness and administration

Cardiology Note:
-------------------
A patient with cancer on chemotherapy, presented to ER with acute coronary syndrome. Is it safe to give him aspirin and clopidogrel knowing his platelet count is only 60,000?
👇🏻👇🏻
"Antiplatelets should not be withheld unless the platelet count is below 10,000/µL for aspirin or 30,000/µL for clopidogrel"
"Experts recommend a minimum platelet count of 30,000/µL for PCI and 50,000/µL for CABG procedures"
----------------------------
Reference:
2022 ESC Guidelines on cardio-oncology developed in collaboration with the EHA, ESTRO and IC-OS
#CardiologyNote
English
Cardiology Note:
-------------------
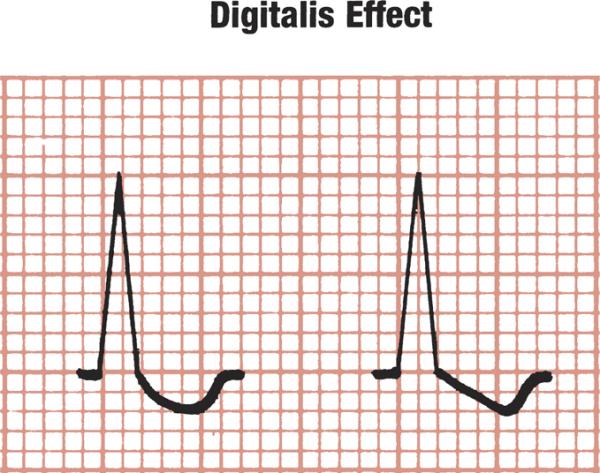
𝗔 𝗽𝗮𝘁𝗶𝗲𝗻𝘁 𝗶𝘀 𝘁𝗮𝗸𝗶𝗻𝗴 𝗱𝗶𝗴𝗼𝘅𝗶𝗻 𝗳𝗼𝗿 𝗛𝗙. 𝗬𝗼𝘂 𝘀𝗮𝘄 𝗵𝗶𝘀 𝗘𝗖𝗚 𝘄𝗶𝘁𝗵 𝗰𝗵𝗮𝗿𝗮𝗰𝘁𝗲𝗿𝗶𝘀𝘁𝗶𝗰 𝗱𝗶𝗴𝗶𝘁𝗮𝗹𝗶𝘀 𝗲𝗳𝗳𝗲𝗰𝘁.
𝗗𝗼𝗲𝘀 𝗶𝘁 𝗻𝗲𝗰𝗲𝘀𝘀𝗮𝗿𝗶𝗹𝘆 𝗺𝗲𝗮𝗻 𝘁𝗵𝗲 𝗽𝗮𝘁𝗶𝗲𝗻𝘁 𝗵𝗮𝘀 𝗱𝗶𝗴𝗼𝘅𝗶𝗻 𝘁𝗼𝘅𝗶𝗰𝗶𝘁𝘆?
👇🏻👇🏻
- A characteristic scooping of the ST-T complex (digitalis effect) sometimes seen in patients taking digoxin
- Notice that in digitalis effect, the ST segment and T wave are fused together and it is not possible to tell where one ends and the other begins (see picture below)
- Digitalis effect can be seen in patients taking therapeutic or toxic doses of digoxin (Not necessarily indicate toxicity)
----------------------------
Reference:
Clinical Electrocardiography: A Simplified Approach, 7th Edition
#CardiologyNote
#MedTwitter
English