@RafidMustafa @MayoClinic Well done guys, I hope this was the first of many, Cheers!
English
Maximiliano Hawkes, MD
293 posts

@mxhawkes
#MayoClinic Critical Care and Stroke Neurologist @MayoClinicNeuro. Tweets are my own.


I am looking to recruit a new postdoc for next year. Please share, thanks! - What: postdoc in population genetics, acute brain injury and chronic cerebrovascular disease. - Where: Yale School of medicine - When: 2/3ys, starting Summer/Fall 2026. Details below! @YaleMed

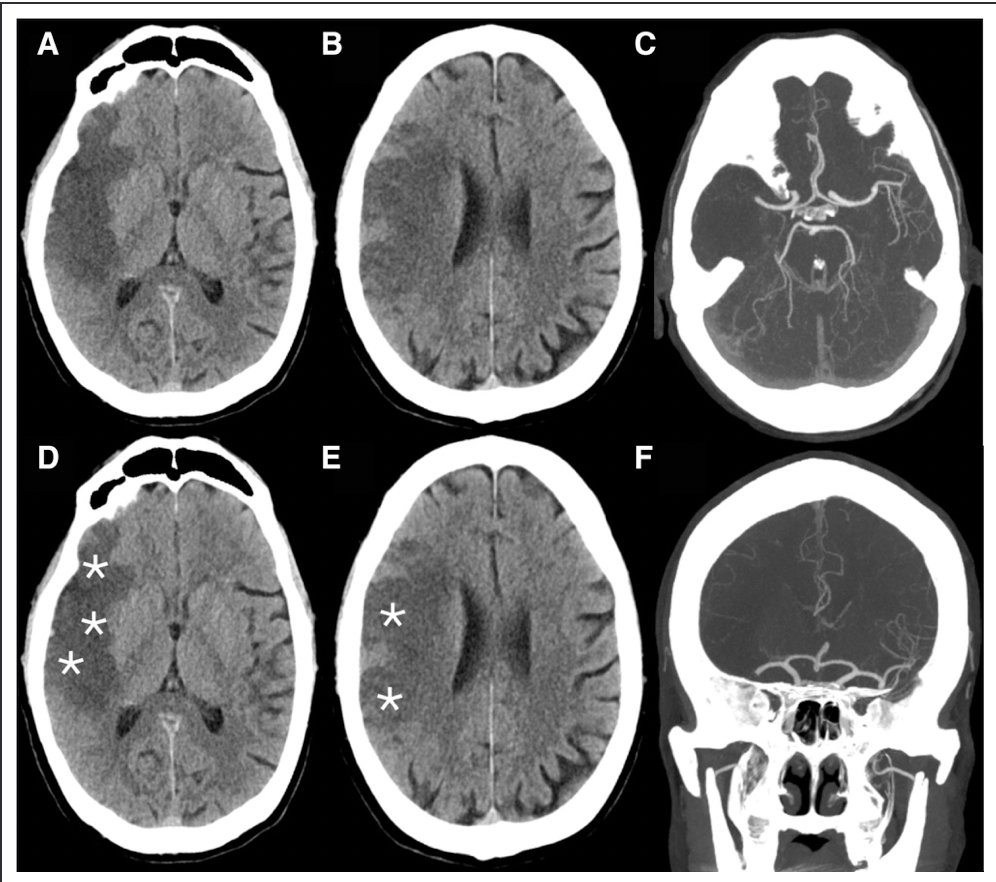





Clocchiatti-Tuozzo et al: Different Responses to Blood Pressure Reduction in Lobar and Deep Intracerebral Hemorrhage Link: link.springer.com/article/10.100… @neurocritical #neurocritcare