@DublinAirport Extremely poor communication with no indications where to wait, and no personnel in place to provide information. Speed it up folks.
English
Vladimir Stoyanov
559 posts

@nephrospot
Nephrologist. Interventional profile. Fluids are not only drinks. Protecting kidneys keep safe hearts and brains. Tweets=personal viewpoints.








KDIGO is pleased to announce the publication of the 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease (CKD). Read the news release: kdigo.co/CKD-Guideline-… Download the guideline: kdigo.co/2024-CKD-Guide… Read the guideline in Kidney International: kdigo.co/CKD-Guideline-… The KDIGO 2024 CKD Guideline was co-chaired by @adeeralevin and @KidneysRU. The Executive Summary will be published in the April 2024 issue of @Kidney_Int. “We are thrilled to publish this eagerly anticipated update, which comes during a transformative period in nephrology, offering new hope for people living with kidney disease," said Dr. Levin. “Recent advancements in GFR evaluation, risk prediction, and the arrival of novel treatments are poised to enhance CKD prognosis and management. We also hope the guideline’s emphasis on multidisciplinary teamwork, patient engagement, and a holistic, evidence-based approach to care will help catalyze positive change, resulting in more coordinated CKD care management worldwide. By integrating the latest evidence and expert consensus, we aim to empower healthcare professionals, and patients with actionable recommendations to optimize patient outcomes and enhance quality of life.” “As Co-Chairs, we would like to recognize the outstanding efforts of the Guideline Work Group and extend our thanks to the Evidence Review Team from Johns Hopkins, without whom this guideline would not have been possible," said Dr. Stevens. "The Work Group was diverse, multinational, highly experienced, and exceptionally committed, and we are grateful for their contributions to both this guideline and to global nephrology.”




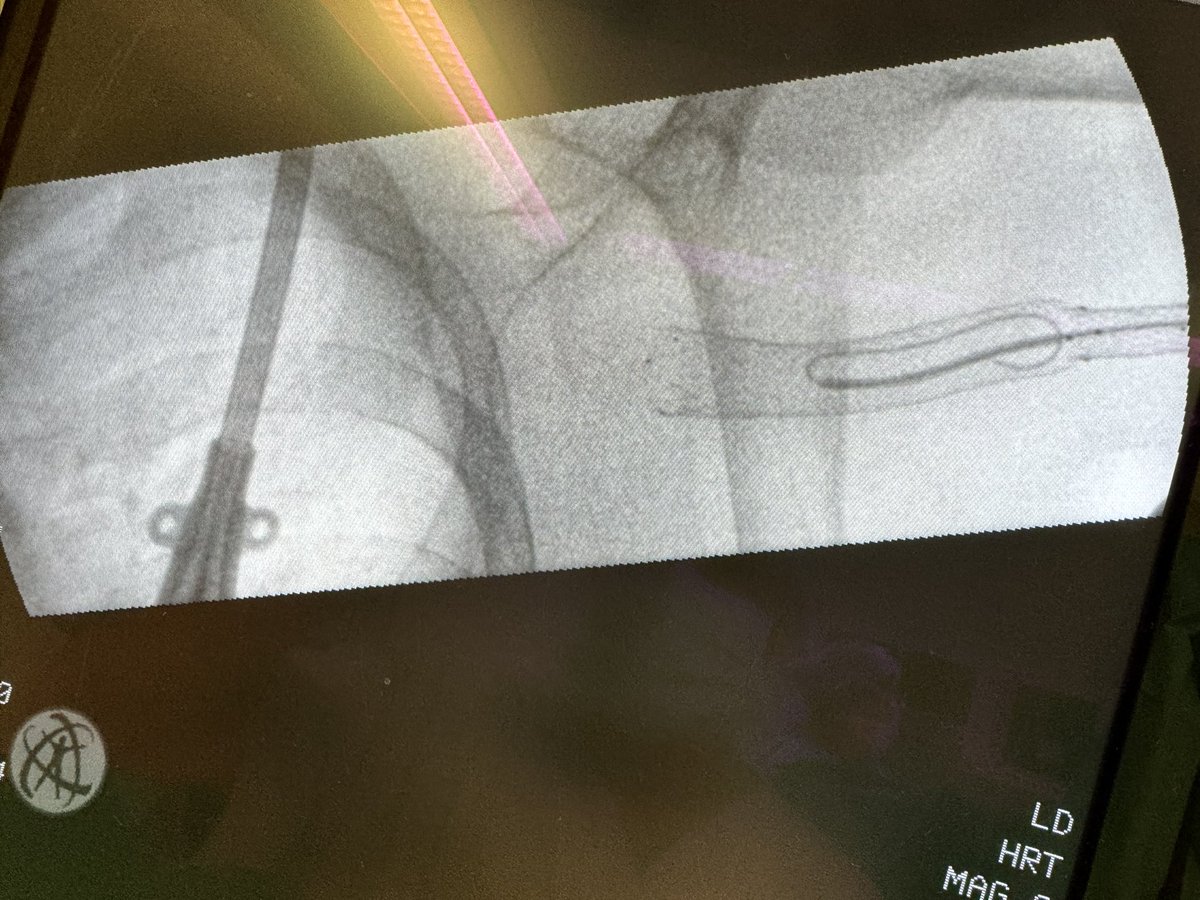
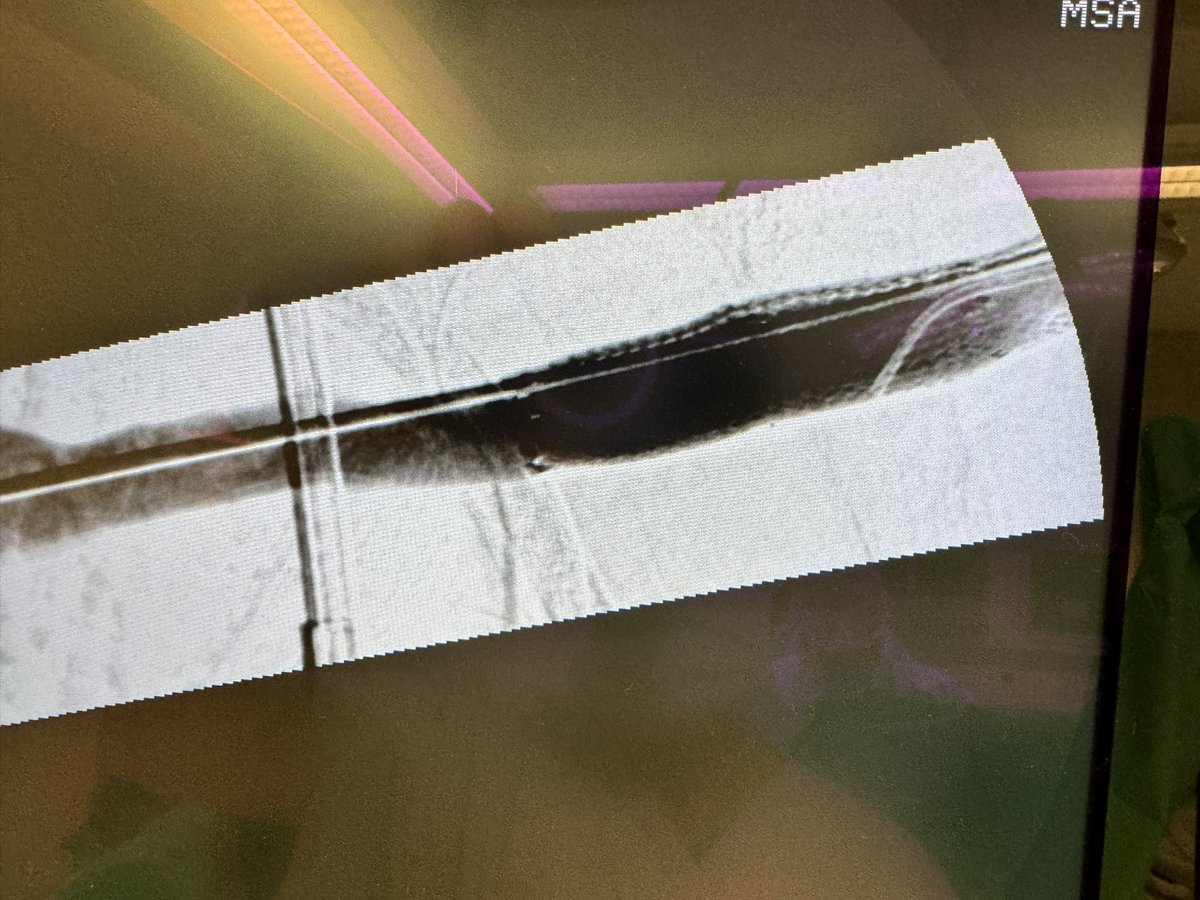
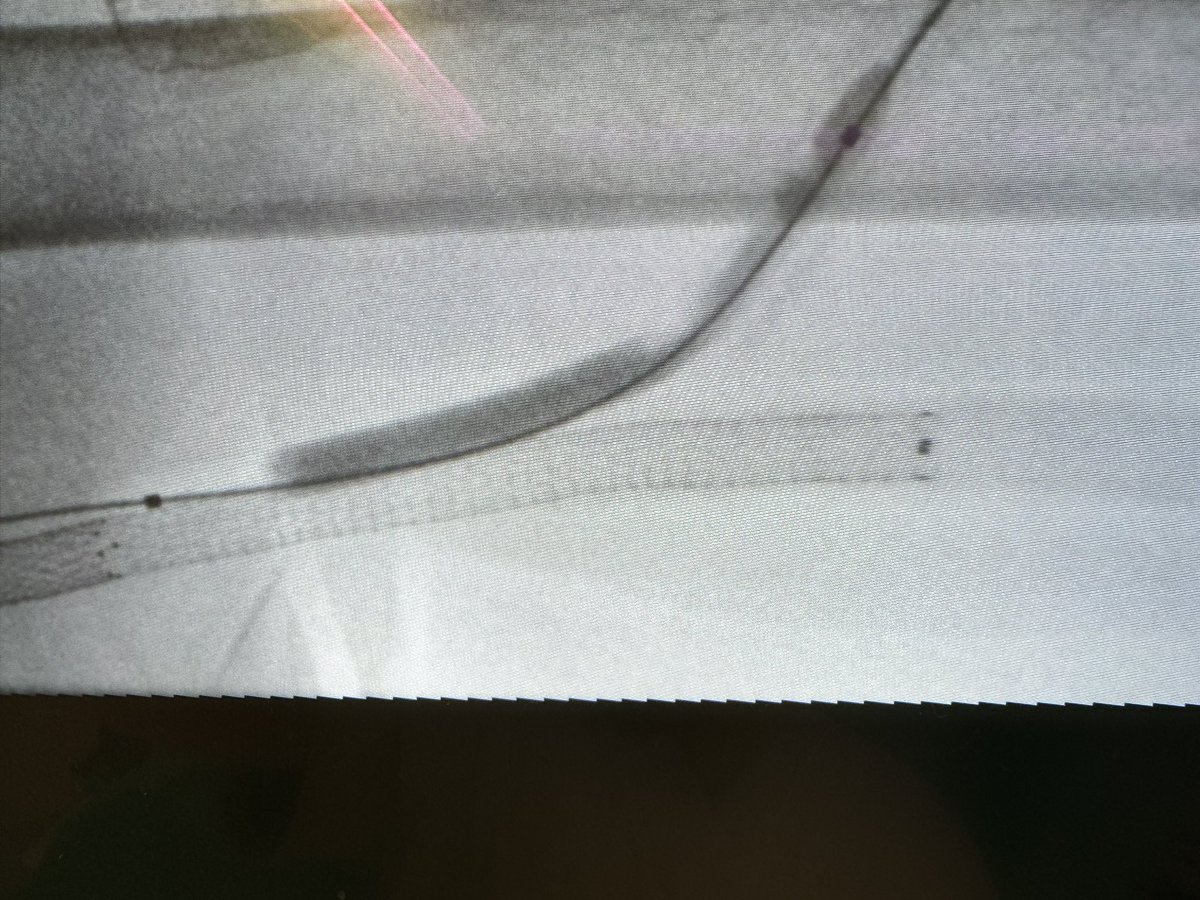
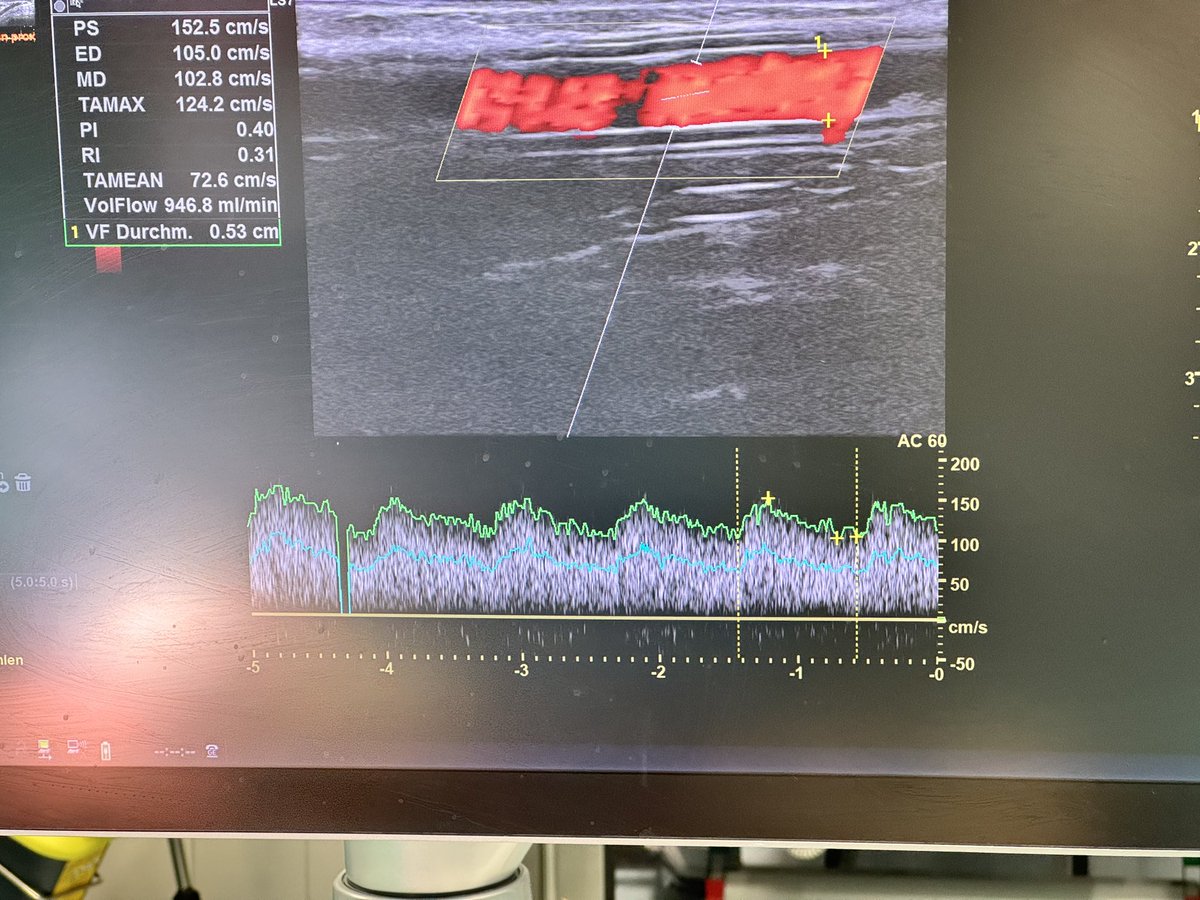
ESRD pt referred for a ‘missing cap” in a RIJ tunneled dialysis CVC. The CVC has been in for FOUR years and the art hub has been exchanged twice. No CRBSI’s. Do you recommend: • Exchanging the catheter for a new one OR… •Repairing the extension/luer-lock