Português
Dr Gabriel Parma. Profesor adjunto de cardiologia
5.4K posts

@parma315
muy felizmente casado y padre de la más linda. amante de la imagenologia cardiovascular . aficionado al fobal y bohemio de corazón , riverense de ley














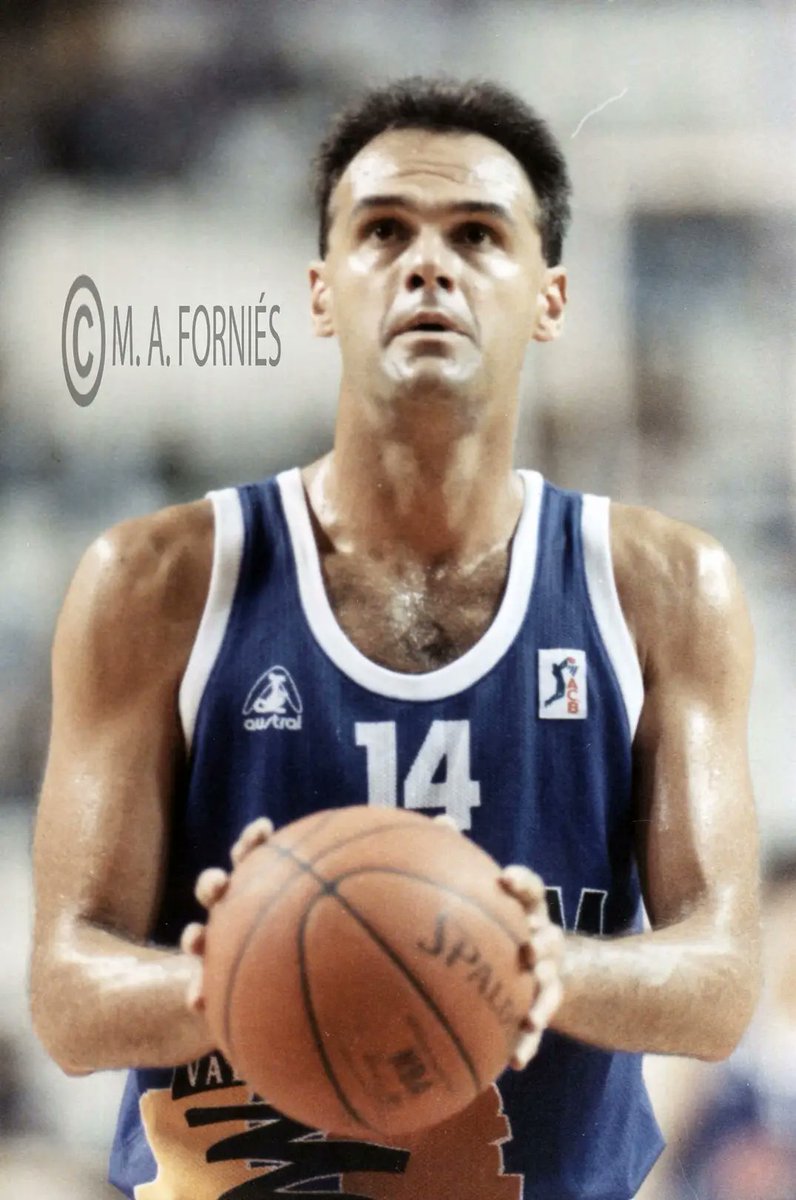



Se va un pedazo de mi infancia , el mejor de los mejores , un animal , no habrá otro igual , esta foto me recuerda todo lo que amo el Basket . Salud campeón