
محمد أبوشويربات
2.8K posts

محمد أبوشويربات
@pure_moh
صيدلاني، ابسط انسان في العالم، فتنة العقل و هدوء المنطق يدهشانه، 🇸🇦
KSA Katılım Eylül 2013
121 Takip Edilen980 Takipçiler


يكون مره باليوم في حالة الارتجاع :
Initial therapy.
Uncomplicated GERD.
Symptoms controlled.
جرعة مرتين باليوم :
اذا كان فيه partial response على مره باليوم
Night time symptoms.
Extraesophageal symptoms.
Erosive esophagitis LA grade C/D.
نعطي IV :
Non variceal upper GI bleeding , esomeprazole 80mg IV loading dose, followed by a 72 hour continues infusion 8mg/hour.
Zollinger–Ellison syndrome.
Sever erosive esophagitis
هذا اللي اتذكره دكتور

للاسف up to date ما عاد يشتغل عندي😢
ابي مرجع لل PPs متى Once Daily ومتى تكون BID لل Oral
ومتى تكون IV وايش ال Indications ومتى once ومتى BID ومتى نعطي Infusion ومتى Bolus
مسااااعدتكم🙏🏻❤️❤️❤️
@MuathSufyani DTR
Difficult to treat resistance pseudomonas aeruginosa
نقدر نستخدم
Ceftolozane – tazobactam
Ceftazidme - avibactam
Català


@usual_unknown @it0z2 التناوب ما هو مُحبّذ
ال national library of medicine
تمنع التناوب من الأساس، و يُنظر فيها فقط بحالة ان شعور الانزعاج طوّل
وفي كتاب OiPiros
مكتوب ان التناوب يكون بالـ pharyngitis فقط
اذا فيه حالات اخرى يُنصح بالتناوب فيها انا مادري صدق
يعطيكم العافية

العربية

Thank you for this precise and scientifically balanced analysis. I completely agree that the clinical context is the key determinant, and that the real challenge in pregnancy cases lies in balancing physiological changes (PK/PD) with the practical reality of treatment adherence (compliance).
In summary, both options (1 mg/kg BID or 1.5 mg/kg QD) are scientifically valid, and the medical decision should remain based on individualization for each patient to ensure the best possible safety and efficacy.
I truly appreciate this valuable insight.
Thank you again 😍🌹
English
In a 65 kg pregnant patient diagnosed with acute deep venous thrombosis (DVT), which of the following anticoagulant regimens represents the safest and most effective therapeutic choice?💊
English
I went through the sources you shared and reviewed the exact statements in context.
From the first source, it states:
“We tend to favor enoxaparin 1 mg/kg once daily mainly because we find it hard to get people to comply with the twice-daily dosing frequency.”
This reflects a preference driven by adherence and practicality rather than a recommendation based on pregnancy specific physiology or comparative efficacy. In pregnancy, prophylactic dosing is typically weight based, with regimens such as 20 mg for <50 kg, 40 mg for <91 kg, 60 mg for <130 kg, and 80 mg for >130 kg, usually administered once daily. Therefore, favoring enoxaparin 1 mg/kg once daily in this context may be misleading, especially if the discussion is about prophylactic dosing rather than therapeutic anticoagulation.
From the second source, the authors report:
“In our propensity score-matched retrospective study, VTE patients receiving enoxaparin once daily had a significantly lower rate of major bleeding and a lower mortality rate compared to twice-daily dosing.”
They also state:
“Patients on enoxaparin once daily had a lower rate of major bleeding (HR 0.16; 95% CI 0.04–0.68) and lower mortality (HR 0.19; 95% CI 0.07–0.54) than those on twice-daily dosing.”
However, it is important to note that this study was conducted in the general VTE population and not specifically in pregnant patients. Therefore, while the findings are relevant, their direct applicability to pregnancy is limited, especially given the distinct physiological changes such as increased volume of distribution and renal clearance.
In addition, the CHEST guideline (9th edition: VTE, Thrombophilia, Antithrombotic Therapy, and Pregnancy) states:
“However, many clinicians use a once daily regimen to simplify administration and enhance compliance. Observational studies have not demonstrated any increase in the risk of recurrence with the once daily regimen over the BID regimen.”
You are absolutely right about the 1 mg/kg BID regimen, as it remains a well established therapeutic approach, particularly in acute DVT. However, clinical decision making in pregnancy should not rely solely on pharmacokinetic changes such as volume of distribution or renal clearance only ( which tend to increase, especially in the second trimester ).
At the same time, this does not exclude the 1.5 mg/kg once daily regimen, as it has shown comparable efficacy in many settings, with potential advantages in terms of adherence, practicality, and ease of administration.
Both regimens are valid, but the key point is that the cited sources should be interpreted within their proper context, and the choice of dosing should be individualized rather than based solely on data derived from non pregnant populations.
English
You are referring to Enoxaparin 1.5 mg/kg once daily, which is a recognized treatment regimen for DVT in some patients.
However, in pregnancy, many clinicians prefer 1 mg/kg twice daily (BID) rather than once daily.
Why BID is Preferred in Pregnancy? Pregnancy changes pharmacokinetics:
Increased renal clearance
Increased volume of distribution
More variable drug levels
Using BID dosing provides:
✅ More stable anticoagulation levels
✅ Less risk of subtherapeutic trough levels
✅ Commonly preferred in pregnant patients with acute DVT
Dose Calculation:
65 kg × 1.5 mg = 97.5 mg once daily
Rounded to 100 mg once daily
This is not completely wrong, but if the question asks for the safest and most effective regimen in pregnancy, then I would go for:
✅ Enoxaparin 60 mg SC BID is the better answer.
Another Practical point:
If you choose the 1.5 mg/kg once-daily regimen for a 65 kg patient, the calculated dose is 97.5 mg, usually rounded to 100 mg once daily.
If a 100 mg prefilled syringe is not available, then you would use the nearest practical available syringe strength or combination according to your institution’s policy (may be you will give (60+40) or (80+20)
ashpublications.org/ashclinicalnew…
sciencedirect.com/science/articl….
English
يعطيك العافية د محمد ع هالمعلومات القيمة ❤️❤️
العربية
من مميزات Ferric citrate في مرضى غسيل الكلى:
يعمل كـ phosphate binder
يرفع مخزون الحديد Ferritin & TSAT
يقلّل الحاجة إلى IV iron & ESAs
يساهم في خفض FGF23 المرتبط باضطرابات القلب والأوعية
ميزة ثلاثية في دواء واحد، لكنه مرتفع التكلفة مقارنة بالبدائل

العربية

اللهم لك الحمد حتى ترضى و لك الحمد اذا رضيت و لك الحمد بعد الرِضـا 🤍
أجتزت بنجاح إختبار الهيئة السعودية للتخصصات الصحية
Officially a licensed Pharmacist!
#SPLE
العربية
@ro7oro7 شكلهم قدموا عرض بمبلغ طفس، يعني جايبين كوتينهو و غريزمن ب ٢٢٠ مليون يورو و مستكثرين ٨٠ مليون على باستوني
العربية


@usual_unknown @westi_ مهنة الصيدلة مظلومة بالعالم كله، و السعودية رائدة بالتطوّر فيها و استحدثت برامج فعّالة تناسب النقلة النوعية القادمة، و دكتور أوس قال في لقاءه مع المديفر ان امكانيات الصيدلي السعودي اكبر من سوق العمل بكبره، الامل بالله اولًا ثم في الصحة القابضة ان الانصاف يكون ملموس
العربية

@westi_ دراسة الصيدلة صعبة وطويلة و تحديداً الاكلينيكية ، يتخرج بتأهيل عالي جداً ولكن سوق العمل لايحتمل هذا التأهيل والمنظومة الصحية ليست متطورة بالقدر الكافي لاستيعاب الصيادلة الاكلينيكيين ، نتج عن ذلك انخفاض حاد في الرواتب و فجوات اخرى لاحصر لها وحسبنا الله ونعم الوكيل
العربية

من اللي شهدته كدراسة أن الصيدلة أصعب من الطب ولو سألت أي طالب طب وش أثقل مادة مرت عليك في سنوات ما قبل التطبيق بيقول لك الفارما، لكنها حقيقة محزنة ولا أعتقد أن المجال يستدعي المقارنة
العربية


السوشل ميديا صايره مو حلوه
كل ما فتحت القى حلطمه
وكل تخصص فيه مشاكل
واحس ما احد مرتاح
احس ال vibes صايره عبارة عن اكتئاب
العربية


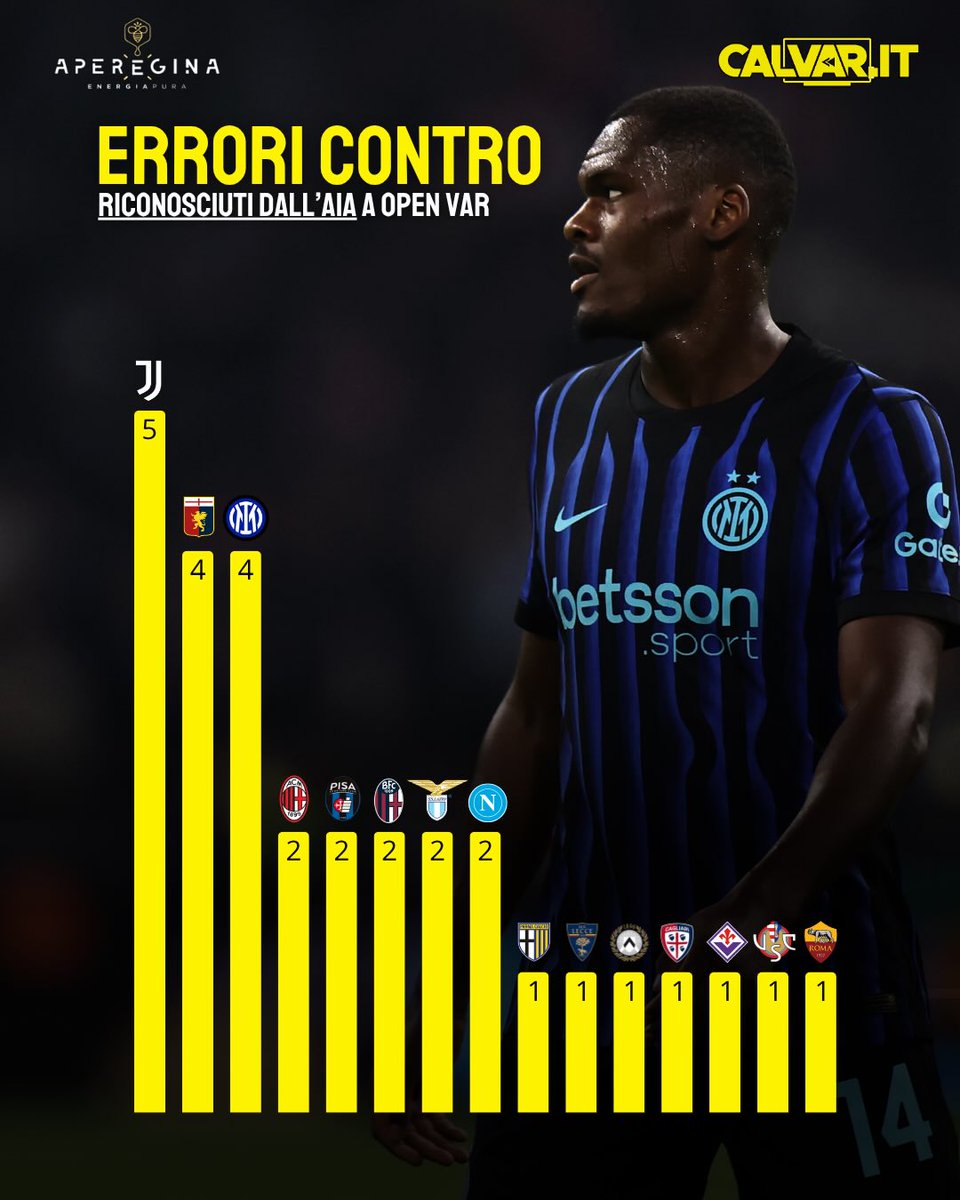
🚨 OpenVar | الأخطاء التحكيمية التي اعترف بها الاتحاد الإيطالي للحكام (AIA) رسمياً لهذا الموسم:
❌ أخطاء ضد الأندية:
• يتصدر القائمة يوفنتوس بـ 5 أخطاء ضده، يليه إنتر بـ 4 أخطاء
✅ أخطاء لصالح الأندية:
• يتصدر القائمة لاتسيو و فيورنتينا بـ 4 أخطاء صبّت في مصلحتهم

العربية
@Dr_Mohammedolog What about with rifaximin in hepatic encephalopathy?
English

*️⃣ لماذا لا يتم إعطاء اي مضاد حيوي مع دواء Lactulose
⬅️ لأن دواء الـ Lactulose يعتبر prodrug ويتحول إلى الصورة الفعالة بواسطة البكتيريا النافعة الـ Normal flora.
⬅️ والمضادات الحيوية تقضي على البكتيريا النافعة والضاره مما يؤدي الى إلغاء فعالية اللاكتيلوز (Lactulose)
العربية