Rafalimumab retweetledi

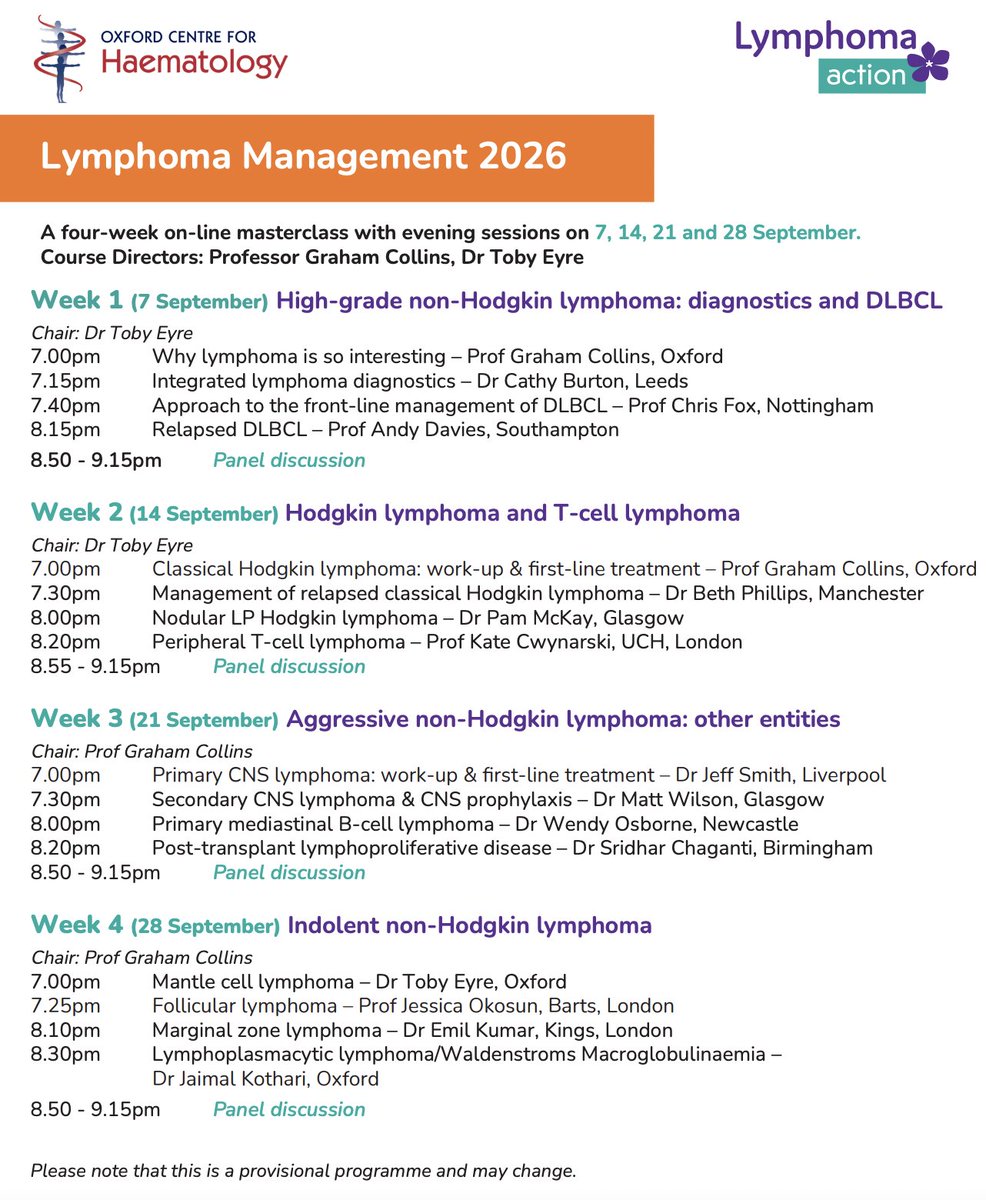
Booking is now open for Lymphoma Management!
- leading event for healthcare professionals
-online course focused on diagnosis & management of lymphoma.
- Webinars delivered virtually on four consecutive Monday nights in September 2026
- Bargain price!
lymphoma-action.org.uk/LymphomaManage…
English