Eze123
17 posts

@DomPosen @avacta @coughlin582 @ICRHealthcare We don't need any more science updates, how tone deaf are you?! We KNOW the science is GREAT, why don't you tell us how you're going to repay your investors for their long-suffering loyalty?
#avct
English

@avacta @coughlin582 @avacta @ICRHealthcare we are excited to hear about new science developments but please also tell us how excited both pharmaceutical reps were during presentations and how much buzz Avacta #AVCT is creating in biotech community, please be as much “commercial” as poss
English

Dr Christina Coughlin, Chief Executive Officer, and Michelle Morrow, Chief Scientific Officer, will be presenting at a webinar on 15 May 2025 at 6.00 pm (BST). turnerpope.com/register/ #AVCT
English

@tim_pass20633 My take:
asininityandbeyond@asininitybeyond
@Tom_The_Bomb__ @SeanDentBsc @avacta @coughlin582 IMO terms already reviewed + agreed, w. settlement of CLN dependent on funds landing imminently They wouldnt RNS about reviewing terms, if not already done or v nearly there. Makes no sense for that to be HCI’s first sight of this My read is something material is very close.2/2
English

Clear why @coughlin582 is so excited.
#AVCT’s AVA6103 indeed looks like a ‘beast’ with complete responses across 19/21 models.
How do @avacta’s brokers value such pre-clinical promise?
Peel Hunt: 14p
Panmure Liberum: 0p

Avacta@avacta
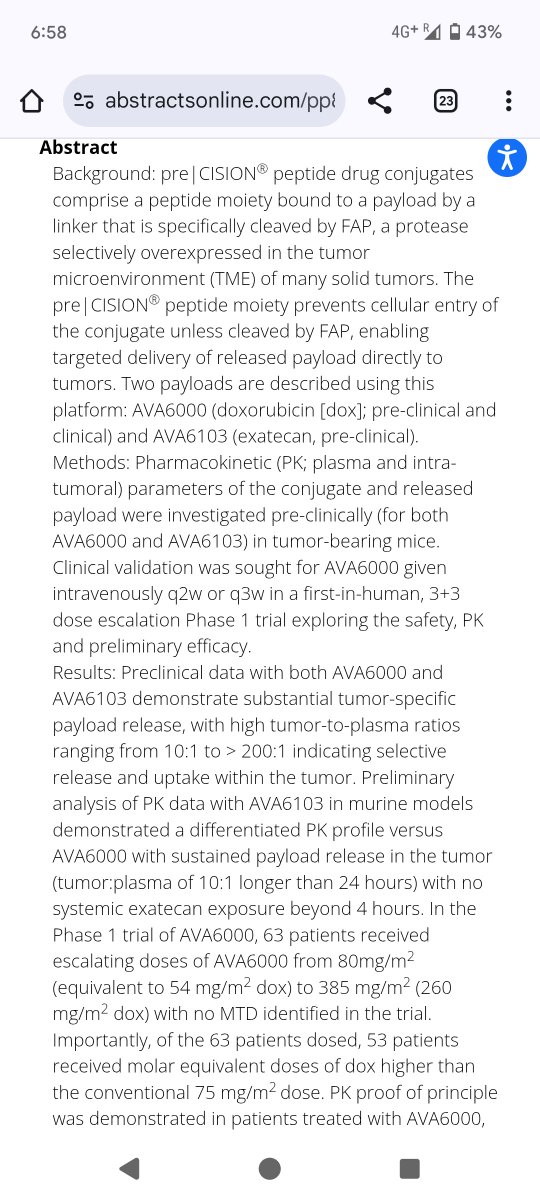
The preclinical and translational data being presented on two posters by the Avacta team today at #AACR25 are now available to view on our website at avacta.com/about/scientif…. A third poster, on safety and efficacy data for AVA6000, will go live at the same time tomorrow. #AVCT
English


@Tom_The_Bomb__ That being said, as with all things #AVCT, they probably need some advice switching the lights on...
English

@tim_pass20633 Yes, it will be very complex. Especially when AIM is currently valuing us at just $150M. Avacta will need support from likes of LEK & Tempus to obtain the big bucks ($XXB).
English
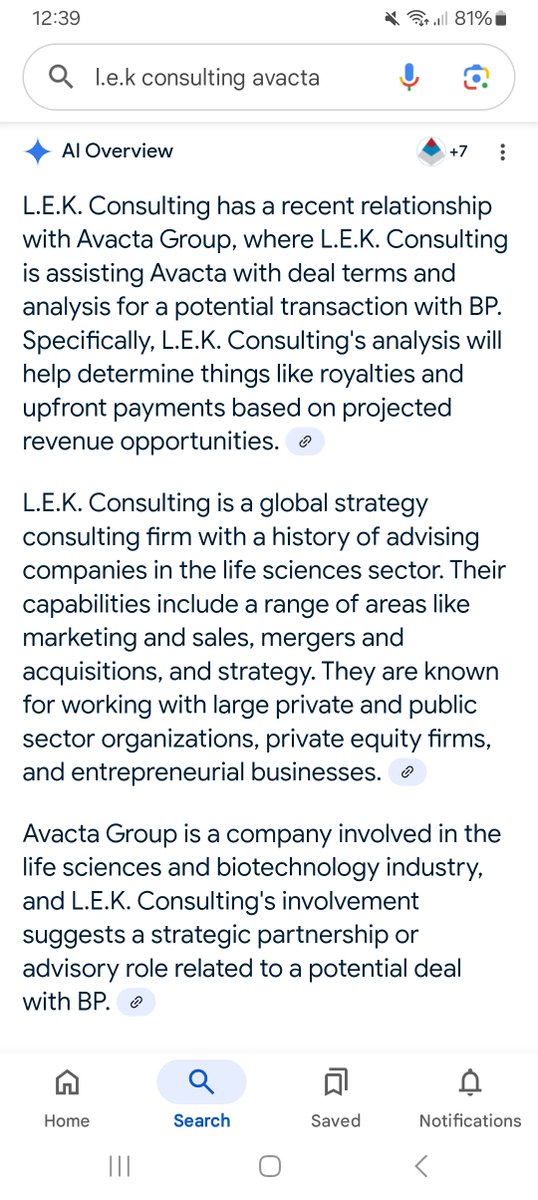
Not sure if this has been highlighted before, but #AVCT is engaged with L.E.K Consulting (see below).
L.E.K is a well known advisor in this space.
Their analysis will help anchor deal terms with BP. e.g royalties, upfront $ based on a modelled revenue opportunities.

English
@Tom_The_Bomb__ There is a complex deal being ironed out in the background, imo. It will not be a simple process to partner pre|CISION with BP, hence the consultancy firm's involvement.
English

@tim_pass20633 @RAH00084 Alastair the guy who sold a load of shares to buy a house? 😂
English
Pharma makes money from supplying solutions to problems. Glib but true.
Within oncology that typically means researching, creating and manufacturing drugs which prevent disease progression.
Drug development is a very costly and lengthy process as #AVCT shareholders are only too aware. It’s also why junior biotechs see such volatility before their eureka moment.
Doxorubicin has been around for 50 years. It may not be the most exciting drug on the market but - for a variety of indications - it is the best available. That includes TNBC (where doxorubicin is often given as a combo therapy).
Until something betters it - which has not happened in 50 years - it will continue to be a mainstay of breast cancer (and many other) treatment regimens.
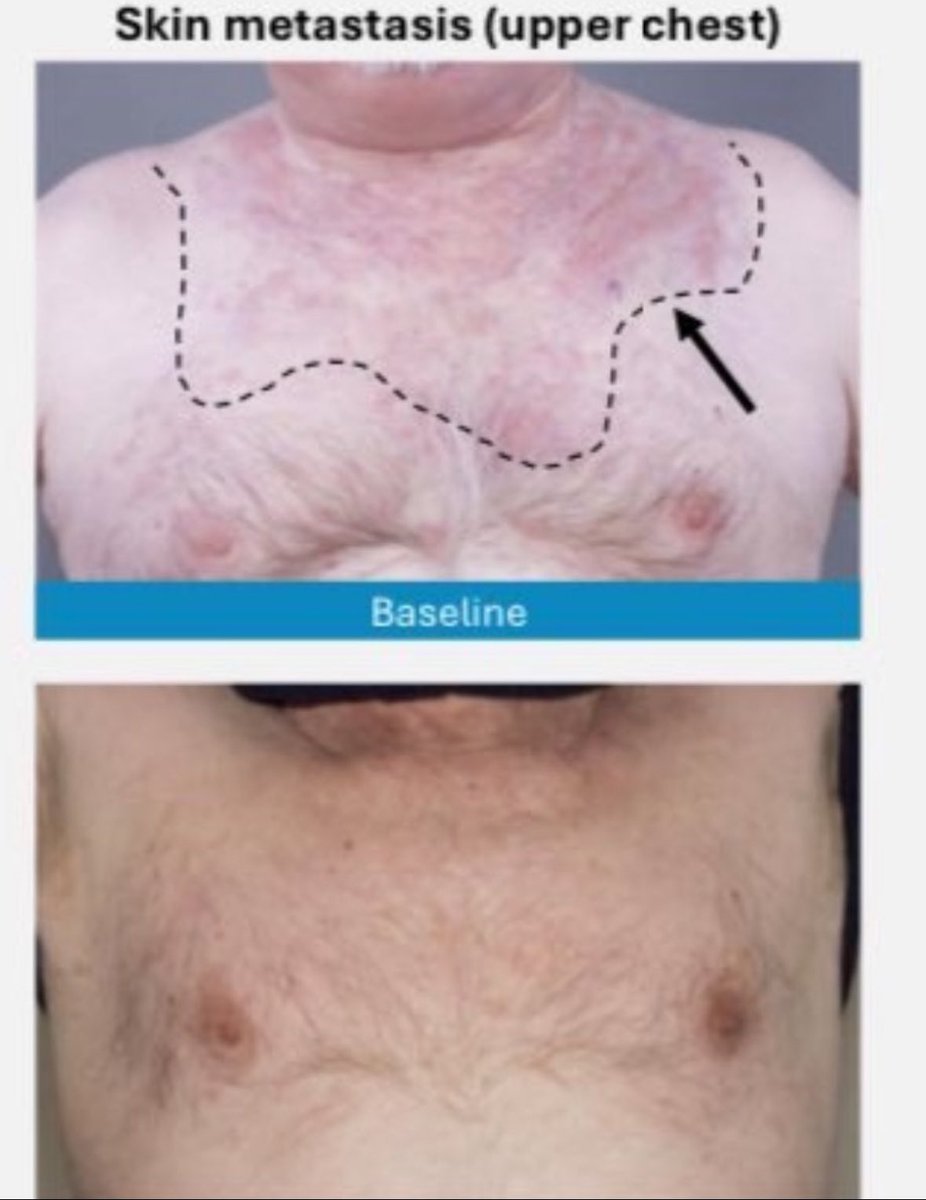
AVCT is supercharging doxorubicin and delivering it safely.
To date, its impact is most acute when you look at the photo of the SGC patient’s skin metastases which saw complete regression after just one dose.
Patients have seen no serious cardiac events as a result of taking AVA6000. Cardiac events typically limit doxorubicin dosing. NB. See V.Sacchini, MSK breast cancer surgeon, clip below.
Salivary gland cancer (SGC) has no standard of care. Clinicians can’t open their book, flick to a page and point to a drug/dose/regimen.
Therefore, if your alternative is a cocktail of drugs to keep SGC at bay vs AVA6000, AVA6000 will be used - assuming it can beat the PFS in this indication. Which AVA6000 is beating to date. This will likely be the endpoint the FDA uses to approve the drug for use.
Solutions in oncology are rare and valuable. AVCT looks to be sat on a potential solution for SGC. That is why the indication is pulling away from the pack.
The potential for AVA6000 in TNBC is way beyond SGC: it’s blockbuster. Doxorubicin works in TNBC. TNBC is high in FAP. AVA6000 works where doxorubicin works.
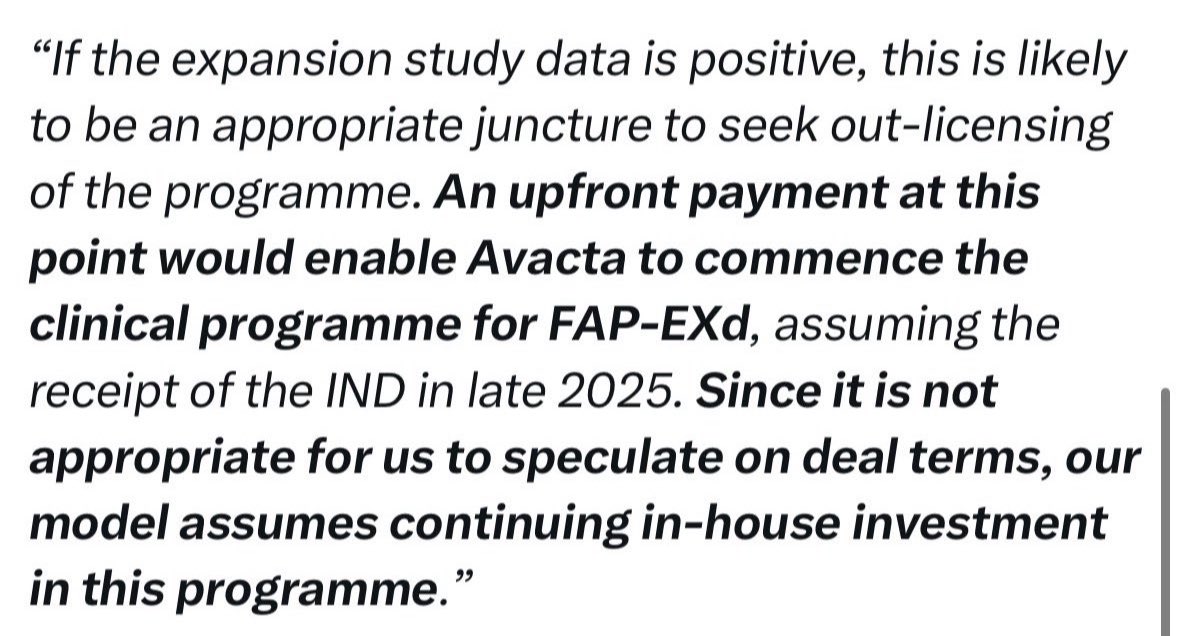
AVCT is currently enrolling TNBC patients onto trial. The broker says the TNBC interim data is the likely trigger for wider out-licensing of the programme.
None of this scratches the surface of the potential of AVA6103 - the preclinical data for which is so good it doesn’t quite look real (so again it is discounted). The broker says this programme has also received partner interest.
The CLN is causing many people to ignore all of this progress.
AVA6000 has been in clinic for 3.5 years. it is delivering a known drug. It is safe. It has dosed 80+ patients. It is keeping people (who have failed other clinical trials) alive. In short, it is working just as Bachovchin intended.
The company is at AACR next week with a larger presence than they have had before. That’s not by chance. It’s a presence justified by the clinical data accumulated to date.
Which begs the question, why has the AVCT board not been able to sell this vision to investors?
The board lacks commerciality. It lacks members who are cognisant of what the exchange (the company reluctantly sits on) demands. It lacks any credible excuse for failing to deliver a solution to the much maligned CLN, which 4/7 current board members signed off on as directors.
You cannot on one hand tell shareholders in Apr 2024:
“The board is working towards the plans to fund all of that innovation... This is a key priority… for the board in the short term. And I will reiterate to you, everything is on the table and we are working together with just a short bit of time here to come back to you on some answers to these questions.”
Then, a year later, blame your commercial environment when you convert in stock, having previously signalled to the market the Dx disposal and dilution were factors in your historic decisions.
Well, you can - indeed the board has - but you should not then be surprised when shareholders begin to question whether the right mix of skillsets sit around the table.
It is very clear bolstering of the board is required if AVCT’s commercial prowess is going to support the clear and vast potential of its technology.

English
@Towlie1981 No one was realistically expecting it to be paid in cash. As M McF said, fewer words would have been the best course of action. Just copy/paste the previous RNSs. Simple. Trying to explain the decision comes across as weak and only serves to irk LTHs. Inept comms again #AVCT
English

Everyone acting as if it wasn't going to be paid in shares. Science still fantastic. Management still poor. Which one is going to win out in the end? I'm going with science, but for less than it should have (due to perpetually bad management). #AVCT
Clyst Saint Mary, England 🇬🇧 English
“And the addition of Seagen brings Pfizer to what Boshoff called an inflection point in its position in the oncology field.”
What an actual inflection point looks like.
#AVCT
FiercePharma@FiercePharma
Pfizer fleshes out oncology strategy, targeting 8 blockbuster cancer drugs by 2030 fiercepharma.com/pharma/pfizer-…
English
Eze123 retweetledi
A patient can have a 100% reduction (ie complete regression) in large metastases but if their lymph nodal lesions shrink by 15%, their quantifiable score under RECIST isn’t going to convey the significance of the metastatic shrinkage for the patient.
As you say, not only was this rapid, it was mid-low FAP in a patient who had exhausted two other avenues.
The significance of this result will be clearer soon, I’m sure.
English
'Rapid and complete regression of.. skin and visceral metastasis.. in a 74yo patient.. low/mid-level FAP expression.. 15% reduction in parotid and lymph nodal lesions continues at.. 12 weeks... began treatment.. September 2024'
Complete, rapid
3 months! - 15%
Mid-low FAP
#AVCT
English