csemen รีทวีตแล้ว

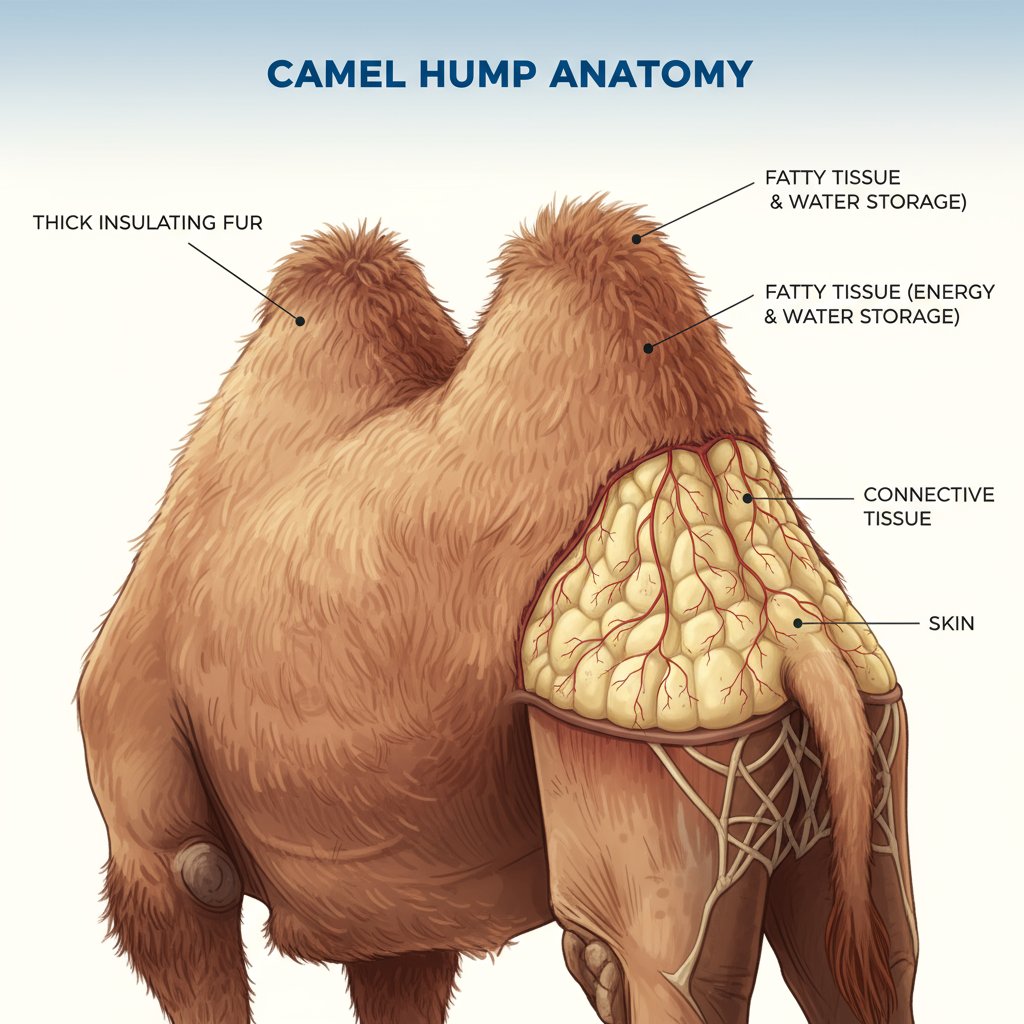
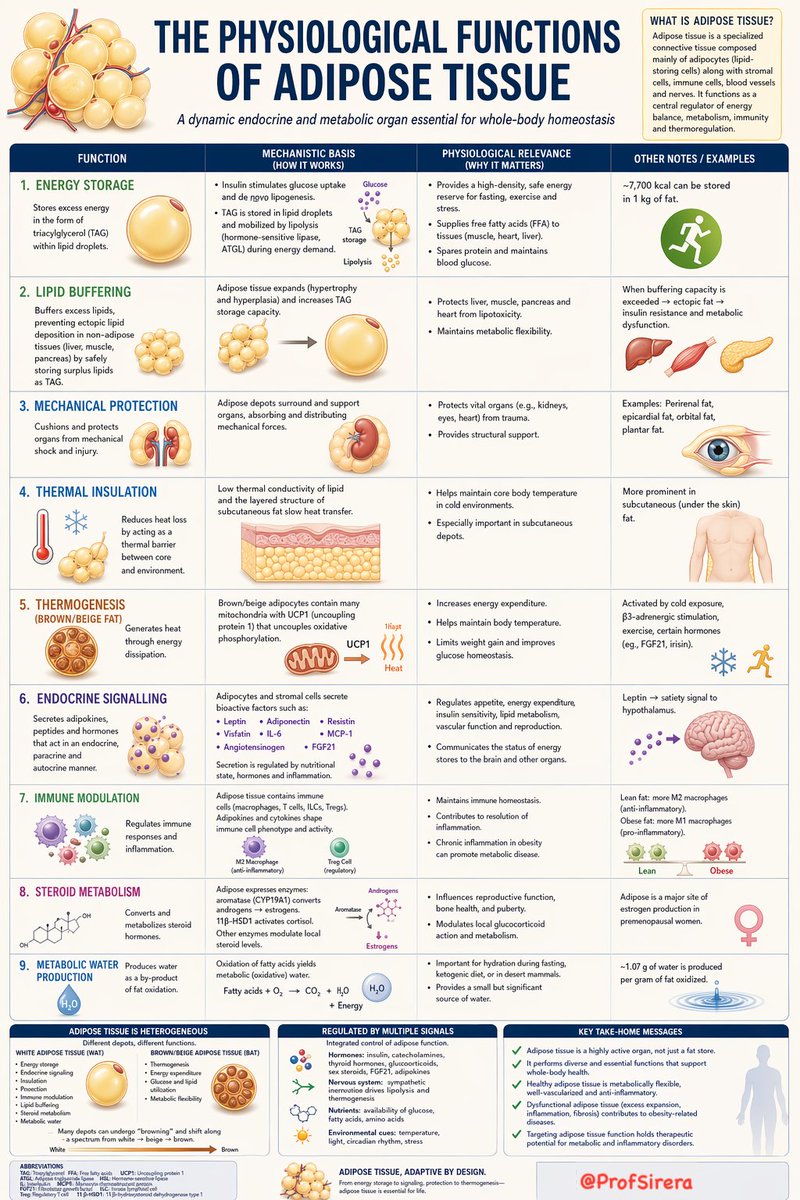
Adipose tissue is not merely an inert energy reservoir, but a metabolically active organ whose diverse endocrine, immune, and regulatory functions are summarised in the following chart.
Note: I was preparing a post and a table to explain the physiological functions of adipose tissue to complement today’s discussion on metabolic water production from fat oxidation (x.com/ProfSirera/sta…), when I recalled that other communicators, such as @drkeithsiau, had used ChatGPT to create remarkably effective posters—so I set to work.
English