ทวีตที่ปักหมุด

Serious systemic adverse effects (beyond package side effects) from #fluoroquinolone (#Cipro/#ciprofloxacin, Levaquin (off market)/#levofloxacin, Avelox/#moxifloxacin etc) antibiotics may persist for extended periods, potentially lasting for years or indefinitely for some.
In 2016 and 2018, the FDA advised that fluoroquinolones should only be used in cases where no other options are available for sinusitis, bronchitis, or uncomplicated UTIs. They contain multiple Black Box warnings,* the most serious warnings a medication can have.
If you are experiencing any or all of these symptoms below and are stunned by the ongoing emergence of new and troublesome issues following the antibiotic treatment you underwent, you have been what is deemed 'floxed':
✅ Extreme weakness, inability to stand or walk as before prescription
✅ Nerve problems — weakness, numbness, pain, muscle jerking and twitching, crawling bug feeling
✅ Tendon tears and muscle weakness
✅ Collagen destruction, hanging skin, wounds slow to heal
✅ Acute sensitivity to sunlight, sudden hormone & thyroid issues
✅ Ringing in the ears, vision disturbances
✅ Anxiety, panic attacks, disorientation, impaired concentration or memory, confusion, depersonalization, hallucinations, psychoses
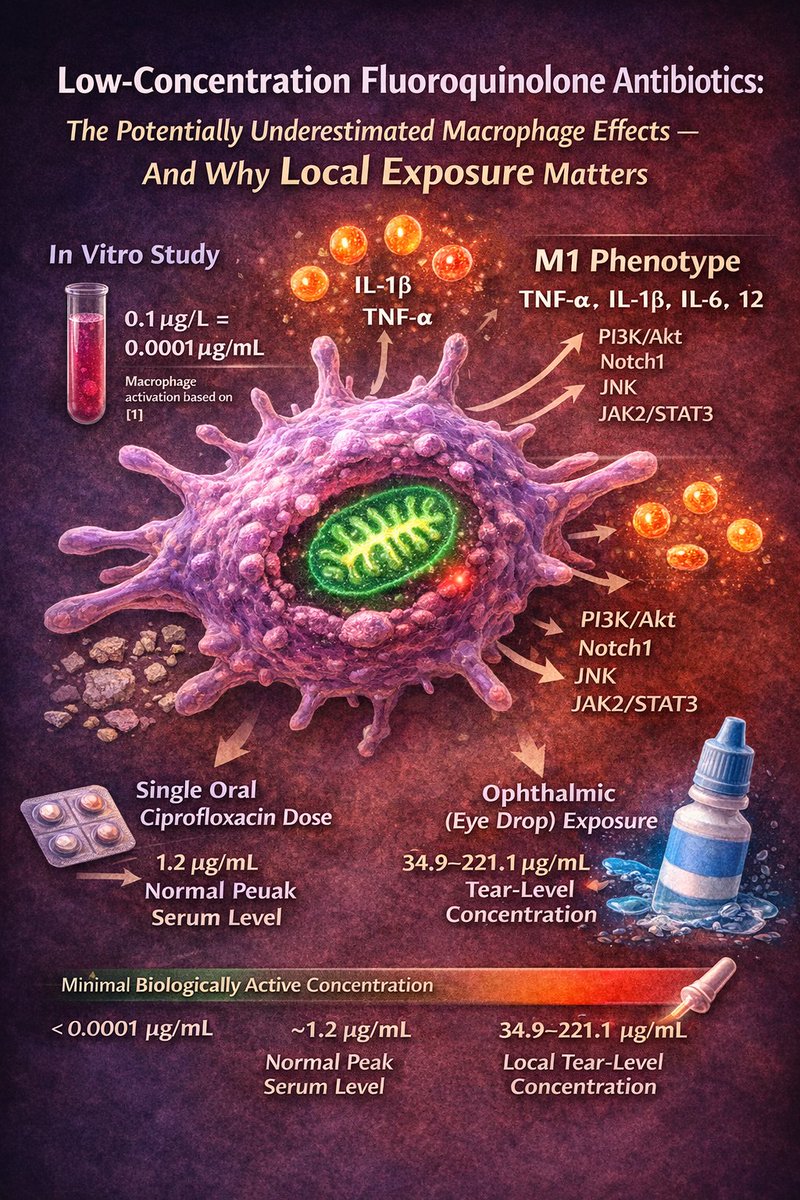
Due to the potential of mitochondria** dysfunction, the actual list of adverse effects can be quite lengthy. Every prescription drug has side effects, some worse than others. Please do your research before you take that next pill, ear drop or eye drop, ask for a substitute if needed - don't let yourself become a statistic.
🟠 🟡 🟢 🔵 🟣 ⚫ 🟤
*Black Box warnings: fq100.org/fda-warnings
**Mitochondria are the powerhouse of your cells
➥Listen to our 3 part series with Dr. Stefan Pieper: YouTube channel: @FqAntibioticDamage" target="_blank" rel="nofollow noopener">youtube.com/@FqAntibioticD…
💊Medications in the fluoroquinolone class (incl: Cipro/ciprofloxacin, Levaquin (off market)/levofloxacin, Avelox/moxifloxacin etc) in all forms for humans and pets: fq100.org/drug-list
Find support and resources on our sites:
🌐 Medical resources: fq100.org/find-medical
🧭 Help & Misc resources: fq100.org/find-help
▶️ YouTube: @FqAntibioticDamage" target="_blank" rel="nofollow noopener">youtube.com/@FqAntibioticD…
🐦 X/Twitter: x.com/fq_100
#FQAwareness #Fluoroquinolones #MitochondrialHealth #AntibioticSideEffects #Floxed #Cipro #Levaquin #FQAD
⚠️Disclaimer: Fluoroquinolone Toxicity Study does not provide medical advice, and all articles and written content are intended for informational purposes only. We do our best to provide accurate information. Such information is not a substitute for professional medical advice, diagnosis or treatment. For multiple reasons, supplements, treatments, and pharmaceutical effects and outcomes can possibly vary significantly among those affected by fluoroquinolone drugs.

English