ทวีตที่ปักหมุด

I’m excited to share a new infographic and podcast discussion stemming from our recent paper on chronic abdominal pain and emergency department utilization using 2023 NHIS data.
The team at @AcademicEmerMed and the Skeptics’ Guide to Emergency Medicine (SGEM) went above and beyond to help translate this research into practice—thank you to the SGEM hosts and the journal for the opportunity to discuss the work and for creating such a thoughtful and visually engaging infographic. It’s rare to see this level of investment in dissemination, and I’m grateful for it.
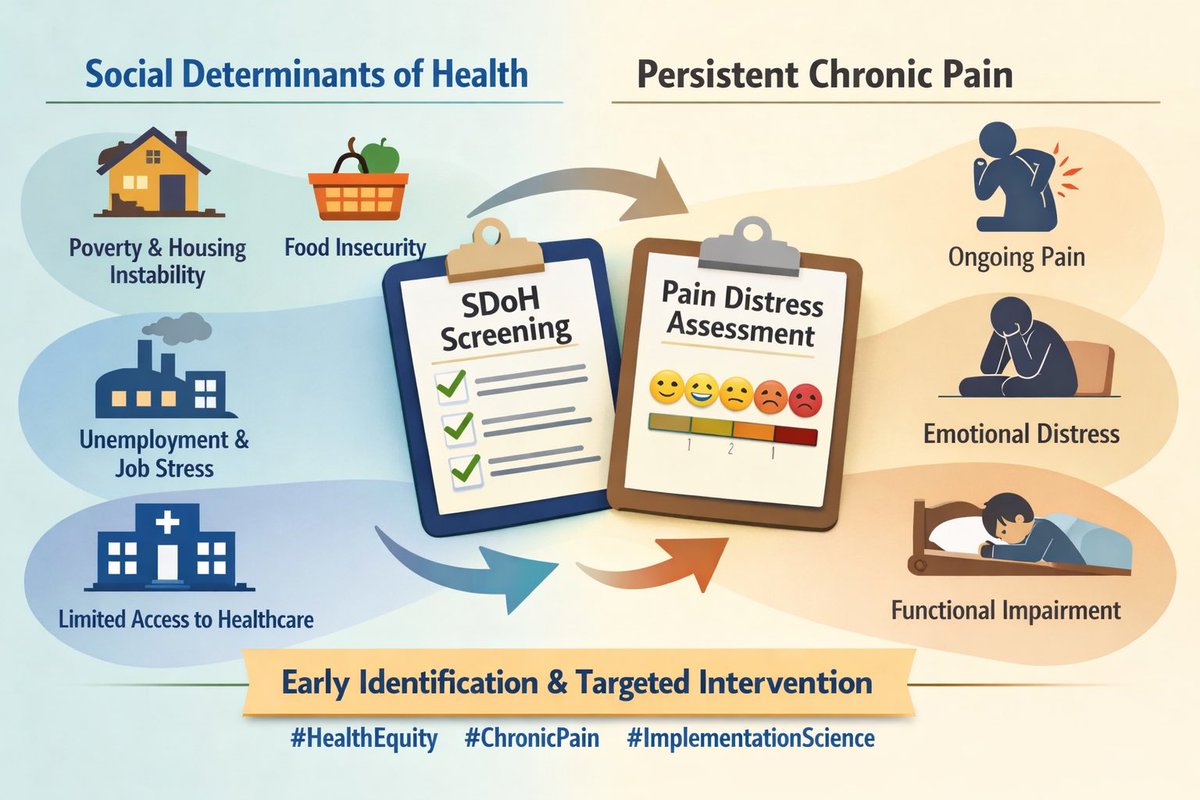
One aspect of this project I’m particularly proud of is the incorporation of social determinants of health. My hope in designing the analysis and writing the manuscript was to highlight how factors like disability status, financial strain, and food insecurity are not abstract concepts—they shape pain experiences, coping, and care-seeking in very real ways.
There is much more to uncover here. And while we are in a moment where I'm often advised to “stay away” from SDOH in grant proposals, the data continue to show how essential these factors are for understanding pain, equity, and outcomes. I remain committed to studying them and advocating for their inclusion in our research frameworks.
If you’re interested, the SGEM podcast episode dives into the methods, findings, and implications, and the infographic beautifully summarizes the key comparisons between people with and without chronic abdominal pain.
Thanks again to SGEM and AEM for helping bring this work to a wider audience.
(Infographic credit: SGEM-HOP #494)
AEM publication: onlinelibrary.wiley.com/doi/10.1111/ac…
SGEM podcast: thesgem.com/2025/11/sgem49…
#EM #Pain #Research #Academic #Clinician

English