NymNymVT
533 posts


NymNymVT
@NymNymVT
A love for the ocean, gaming, and art! I'm here to share my interest with you and find others to connect to and have a good time. I am an ADULT fyi
The Ocean เข้าร่วม Ağustos 2023
100 กำลังติดตาม28 ผู้ติดตาม
NymNymVT รีทวีตแล้ว


God jkjk ((Idk why I suddenly thought God I just thats all my mind went to))
ChocoCoTV 🐭 Mouse Vtuber@Chococo_TV
If "Mama" is the Model artist and "Papa" is the Rigger. Then what do we call the Character designer?
English
NymNymVT รีทวีตแล้ว

Let’s talk about something that’s really annoying in medicine: Prior Authorizations! 🗒
It’s no lie that medicines and treatments can be expensive. Some pills or infusions can be extremely costly to manufacture, or a super niche custom cochlear implant that costs upwards of 6 figures to create, or paying the surgeon putting that device in through a very complex and delicate procedure. At the end of the day, the system does not expect all people to pay out of pocket for their medical care, and thus many of us pay for healthcare through our medical insurance. But sometimes, the insurance companies end up becoming the arbiters of our care, not the physicians.
For example, let’s take a look at hyperlipidemia (“high cholesterol”). This is a condition that has been linked to increased risk for heart disease, stroke, and vascular disease. So of course, besides lifestyle changes, we have medicines to address that! Statins like simvastatin (Zocor), atorvastatin (Lipitor), or rosuvastatin (Crestor) are great medicines that can significantly lower cholesterol levels, and are taken by mouth once daily. We’ve had them around for decades now and understand their side effects quite well. Your parents are probably on one too! A 1-month supply of generic simvastatin generally costs someone $5 without insurance. They aren’t perfect medicines, but they are affordable and make a significant impact in the lives of a lot of people.
In the past 20 years, science has progressed and we now have an injectable biologic called evolocumab (Repatha), a human monoclonal antibody specifically directed at the PCKS9 protein. Normally PCKS9 degrades LDL receptors in the liver, so it reduces the available amount of LDL (“bad cholesterol”) that can be cleared from the blood. By blocking PCKS9, the LDL receptors stay out in the liver and can continue to do their jobs. Repatha is a great medicine, and shows significant cholesterol-reducing effects when compared to statins. But as you can probably imagine, as an injectable it is more expensive to make and administer. A one-month supply of biweekly injections costs about $800 without insurance. A year of treatment would cost $9600. Probably not affordable for most people.
So this is where insurance is supposed to help, right? After all, you sacrifice a cut of your paycheck to them so that they can help out with the costs of your medications. Well, they need to determine if THEY think that’s a good idea too. Sure, I can write Repatha prescriptions all day because I know that they’re OP compared to sending someone out on statins. But is that realistic? Will your insurance company actually play ball? Enter the prior authorization.
The concept here is about “medical necessity.” Does everyone need to get that super expensive $800/mo medication? Could someone instead be reasonably treated with statins and have just as good improvements? This is where prior authorizations were born, as a utilization management process to discourage healthcare spending on expensive, low-value services. Another example: in the past few years GLP-1RA’s like semaglutide (Ozempic) or tirzepatide (Monjaro) have been the hot new thing for weight loss, even being advertised as a “skinny shot” by celebrities on TV. Yes, there are clear medical benefits to taking these ranging from conditions like diabetes, to sleep apnea, to general weight loss in the obese patient. Imagine you hear this on TikTok or see an ad on the subway, so you ask your doctor for a prescription and they say sure. Then you take it to the pharmacy who runs it against your insurance, and surprise! They’re not going to cover that Wegovy prescription and now you’re on the hook for $300 a month.
Prior authorizations are just as much about convincing the insurance company that the patient requires this treatment, as much as you convincing the doctor that you need the prescription. For better or worse, companies like United or Aetna are like you, just trying to save money. So when they get a request for covering someone’s Wegovy in a patient who technically has a BMI >30, but has no history of making dietary changes, sticking to an exercise routine, no formal sleep study done, and no other comorbidities? They will determine that prescription medically unnecessary, and drop a rejection notice in your mailbox. You can always pay that $300 a month prescription, but your insurance company won’t be helping you.
It’s important to know that a lot of this depends on the doctor’s office doing their due diligence, too! When they send over your records as part of a prior auth, they need to submit the relevant evidence to “prove” that you need the medication. If they are negligent in documentation, or just don’t have these things, then how is the insurance company to know? What if you followed a nutritionist in a different health system and had documentation that traditional dieting wasn’t helping you lose weight? Or what if you did have that sleep study done in another state and you never got the records to the new doctor’s office? Prior auths are finicky, overdetailed, and honestly slow as hell with how long they take to process on each end, so minimizing back and forth transmissions each step of the way counts.
And that’s my problem with them: these things can take an excruciating amount of time to get done. Maybe a couple of weeks of back-and-forth is not a huge deal for cholesterol or weight loss medications, but what about chemotherapy for cancer? Or debilitating conditions like migraines? Even in the inpatient setting as a hospitalist, I am still finding myself doing prior authorizations to get people approved for inpatient therapy, which is just ridiculous to me in the acute care setting. I already have a patient here with severe TTP refractory to 5 days of plasma exchange, why the heck do I also have to write an essay to the CMO on getting them rituximab!? Even expedited submissions and reviews take time, and not everyone can afford that. Surveys have shown that almost 25% of physicians feel that lengthy prior authorizations have led to adverse patient outcomes, including hospitalization, disability, and death. Almost 90% of oncologists report treatment delays because of prior auths, and 75% of them noted that patients routinely expressed worry over delays in their care.
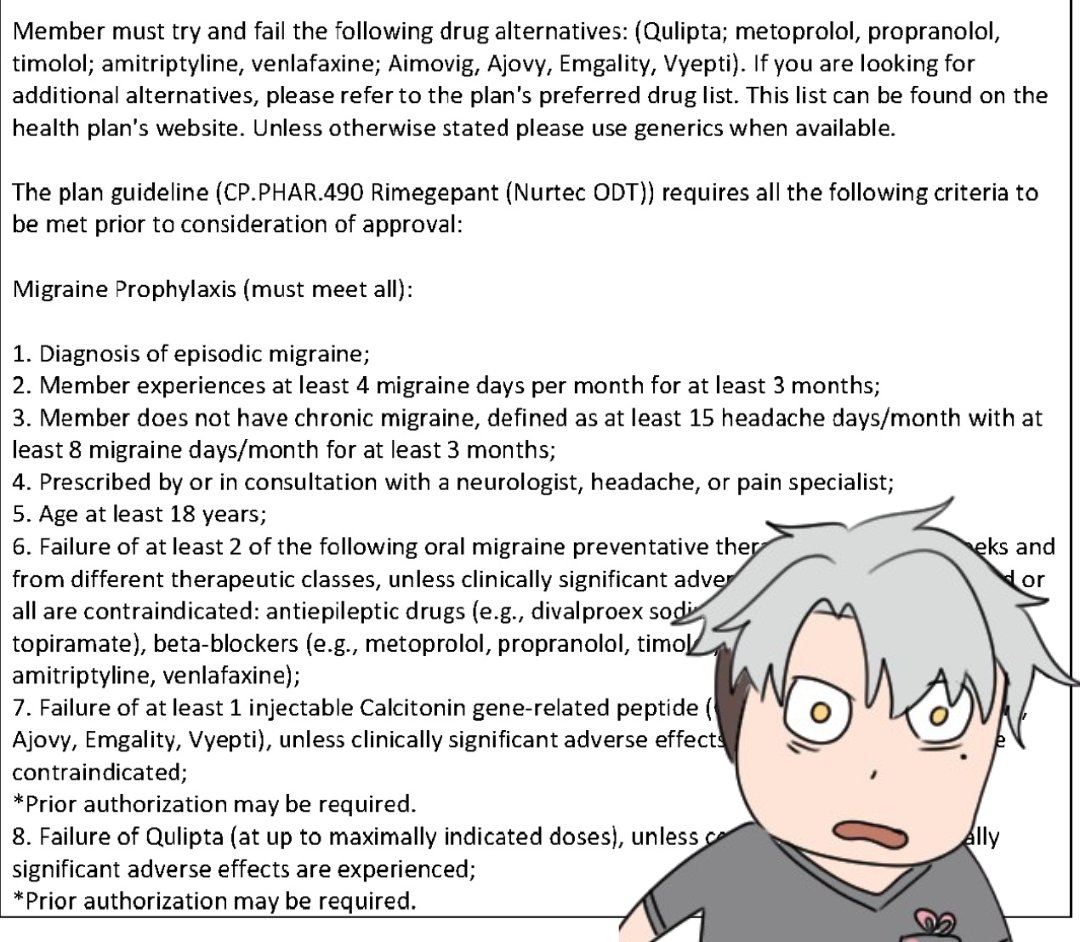
For protracted prior authorizations, delay can lead to suffering and harm. The attached picture is from when I was still doing PCP work in residency: it’s an insurance prior authorization for rimegepant (Nurtec). I had a patient who had been living with migraines for many years and had tried multiple therapies in the past, to no avail. Her sister had recently made huge improvements with Nurtec, and she wanted to see if she could get started on the medicine, too. She had great insurance and a history of the condition with multiple failed medication courses, so I told her we could submit the prior auth and see what happened. After all, from my notes I could say she had episodic migraine at least 4x a month, distinctly not chronic migraine, diagnosed by a neurologist she had seen previously, she had failed traditional therapies, including beta blockers, SNRI’s, topamax, and valproate. I diligently documented her history, compiled all of our clinic notes together, and sent it out.
A week later, they gatekept her: she hadn’t failed enough for them to justify helping out with the Nurtec. Per her insurance, she needed to fail those oral migraine therapies after a period of 8 weeks, not 4. She also needed documented failure of another CGRP injectable like erenumab (Aimovig) or galcanezumab (Emgality). She also needed another documented failure of Quilipta at maximally tirated doses, too. And THEN, would they consider helping out with a PART of the cost of the Nurtec. So we were essentially back at square one, and I had to treat her migraines with medications that her neurologist had already stopped because they had had little benefit, but for 8 weeks instead. Because that’s what her insurance wanted to see! And guess what, Aimovig, Emgality, Ajovy, Vyepti, and Quilipta ALL require prior authorizations of their own, too! So I was filling out prior authorizations within prior authorizations, to get this prior authorization done for the one medication I wanted to get my patient.
This process took the entirety of my PGY-3 year to get through. She continued to have minimal improvement with these therapies, and continued to complain about her migraines. I had to document every single visit her protracted suffering and continue her medications each until we could demonstrate failure per the insurance’s definition. It took nearly 40 weeks for her to finally get approved for Quilipta after all this work. 4 weeks after that, I graduated from residency and moved on from my continuity clinic. I don’t have access to that system anymore to check up on her.
Prior authorizations save money on a system level, and generally do good work in keeping unnecessary treatments from being overkill on a patient’s condition and their wallets. I just wished the system trusted the doctors more to make these decisions themselves and gave them the power to override them. The time and patient suffering just hurts too much on all sides. And don’t even get me started on Peer-To-Peer calls…
Sometimes I still think about if my patient ever got her Nurtec.
English
my resent hobbies a little bit about work what my plans are for the week, talk about games im playing or are currently playing during stream things like that !! what I ate for dinner even?! I like to chit chat
Adriel Reinsley 🦌🍷DOKOMI 2026@Adriel_Reinsley
Vtubers that work a 9 to 5, WHAT THE FUCK do y'all talk about on stream. My just chatting session lasts about 1 hrs and yesterday I ran out of things to saaayyy.....and all I do during the day is make calls and file papers 😭
English
NymNymVT รีทวีตแล้ว



they doing ARGs now and I love that for them
Azahiara@azahiara
Este video se publicó unos segundos en la cuenta oficial de Genshin Impact, luego fue borrado. Columbina está caminando en dirección opuesta a la que vimos en el livestream, perdiendose en la oscuridad. Si me preguntan, va hacia el pasado.
English
NymNymVT รีทวีตแล้ว

