
Simin
450 posts


Simin รีทวีตแล้ว

Hi #PathTwitter 👋
I’m Gelavizh (Gela) Keshtmand, MD, an AP/CP pathologist from Iran, excited to apply for #PathMatch2026 and continue learning in this inspiring field 🔬💜
Grateful for this journey and looking forward to connecting with mentors & colleagues! ✨
#Match2026 #MatchToPath #Path2Path #WomenInPathology #IMGPathologist

English
Simin รีทวีตแล้ว

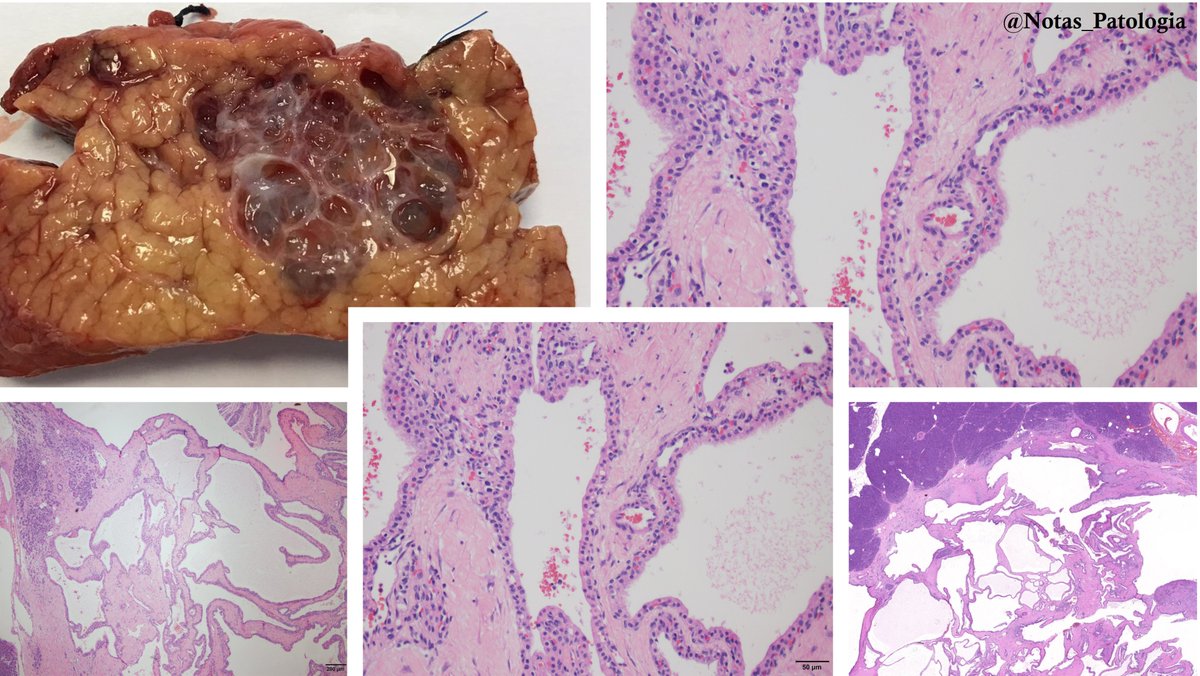
🔬 Serous Cystadenoma of the Pancreas: What You Need to Know
Serous Cystadenoma of the Pancreas, also known as Microcystic Serous Adenoma, is a rare benign cystic neoplasm that shows a female predominance (3:1), typically diagnosed around the age of 58. It accounts for about one-third of primary pancreatic cysts.
🧬 In some cases, it may be associated with von Hippel-Lindau (VHL) syndrome, particularly when multifocal.
📍 Anatomical Location:
Most frequently found in the tail of the pancreas, with a body/tail to head/neck ratio of about 1.6:1. In VHL-associated cases, it may involve the entire pancreas.
🔍 Gross Features:
These are usually well-circumscribed lesions, averaging 6 cm in size but ranging from 1 to 30 cm. The most common type is microcystic, with a sponge-like appearance composed of numerous small cysts filled with clear fluid. Other types include:
Oligocystic (Macrocystic): fewer, larger cysts
Solid variant: homogeneous, gelatinous, and yellow-beige in appearance
A classic feature is the presence of a central stellate scar, consisting of hyalinized fibrous tissue. Hemorrhage may occasionally occur. Multifocality is rare but more common in VHL patients.
🔬 Microscopic Findings:
Cysts are lined by cuboidal to low columnar epithelium with clear cytoplasm rich in glycogen (PAS-positive, diastase-sensitive).
Nuclei are round, uniform, with dense chromatin, inconspicuous nucleoli, and no mitoses.
The stroma may range from edematous to fibrous, sometimes myxoid or hyalinized, and features a rich capillary network. Calcifications can be present.
Variants include tiny papillary projections (without fibrovascular cores), oncocytic types with granular cytoplasm, and a solid variant with compact small glands and minimal lumina.
🧪 Immunohistochemistry:
Tumor cells are typically positive for EMA, MUC1, pancytokeratin, inhibin, and GLUT1, and negative for HMB45. These markers help distinguish it from other cystic neoplasms.
🧬 Molecular and Cytogenetics:
VHL gene alterations are common, especially in VHL patients, with loss of heterozygosity on chromosome 3p. Similar findings can occur in sporadic cases, suggesting a genetic component in tumorigenesis.
💧 Cyst Fluid Analysis:
Fluid is typically low-viscosity, with low amylase and CEA (<5–20 ng/mL). Cytology shows cuboidal cells with glycogen-rich cytoplasm. In VHL patients, VHL gene mutations may be detected.
📈 Prognosis:
This neoplasm is almost always benign, with slow growth (median 0.29 cm/year). The malignant transformation risk is <3%, and associated mortality is virtually nonexistent. Large tumors may compress adjacent organs but rarely pose significant clinical concern.
📌 Clinical-Pathologic Summary:
Rare benign cystic neoplasm, mostly in middle-aged women
Preferentially located in the pancreatic tail
Characterized by clear fluid-filled microcysts and central scar
Cuboidal epithelium with glycogen-rich cytoplasm and bland nuclei
Immunopositive for EMA, MUC1, GLUT1
Associated with VHL gene alterations
Excellent prognosis with minimal malignant potential
📚 References:
Pathology Outlines – Serous cystadenoma
StatPearls – Pancreatic Serous Cystadenoma
Am J Surg Pathol 2015;39:1597 (PMID: 26559376)
J Gastrointest Cancer 2010;41:197 (PMID: 20140653)
Pancreatology 2009;9:182 (PMID: 19077470)
Ultrastruct Pathol 2006;30:119 (PMID: 16517478)
World J Surg 2003;27:319 (PMID: 12607059)
Dig Surg 2016;33:240 (PMID: 26998825)
Am J Pathol 2001;158:317 (PMID: 11141506)
📌 Disclaimer: This content is intended for healthcare professionals and is for educational and informational purposes only. It does not replace individualized clinical evaluation, medical judgment, or institutional guidelines. In real-world scenarios, specialist consultation and updated evidence-based protocols are essential.
#SerousCystadenomaOfThePancreas
#MedicalEducation #NotasDePatologia
English
Simin รีทวีตแล้ว
🔬Uterine Tuberculosis (UTB): An Under-recognized Cause of Infertility
🔬 What is it?
Uterine tuberculosis (UTB) is the infection of the endometrium by Mycobacterium tuberculosis, usually via haematogenous spread from a pulmonary focus. It represents the most common form of female genital tuberculosis (FGTB), affecting the endometrium in ≈ 50–80 % of FGTB cases and causing infertility in 40–50 % of patients—especially in regions with a high TB burden such as India.
Clinical Impact
Typical profile: Women of reproductive age, often with primary infertility or long-standing menstrual disturbances (amenorrhoea, oligomenorrhoea, menorrhagia).
Late sequelae: Intra-uterine adhesions (Asherman syndrome), reduced endometrial receptivity, increased risk of ectopic pregnancy (33–72 %). Only sporadic spontaneous pregnancies are reported after treatment.
Assisted conception: IVF success rates vary widely (≈ 16–38 %), largely depending on endometrial integrity; baseline FSH tends to be higher and live-birth rates lower than in other infertility cohorts.
Diagnostic Approach – Why It Is Challenging
Imaging
HSG: “Beaded” or “T-shaped” cavity, filling defects or “glove-finger” tube outline.
Ultrasound/MRI: Heterogeneous or thin endometrium, intra-uterine synechiae, hydrosalpinx.
Histopathology
Endometrial biopsy/curettage (ideally late luteal phase): non-caseating or caseating granulomas with Langhans‐type giant cells. Sensitivity ≈ 50 % because menstrual shedding may remove granulomas.
Bacteriology & Molecular tests
AFB smear: low yield (< 10 %).
Culture (L-J, MGIT): positive in 5–8 % of endometrial samples; takes weeks.
PCR / GeneXpert MTB/RIF: high analytic sensitivity (< 10 bacilli mL⁻¹) and specificity but prone to false positives; GeneXpert data for FGTB still limited.
LAMP assays: sensitivity ≈ 66 %.
Endoscopy
Hysteroscopy may reveal pale cavity, caseous nodules, “starry sky” tubercles, dense adhesions. Should be performed by experienced surgeons, often under laparoscopic control.
Standard Therapy & Outcomes
First-line regimen: 2 months HRZE → 4 months HR (isoniazid, rifampicin ± ethambutol). Clinical–microbiological cure rates reach ≈ 95 %.
MDR-TB: 18–24 months with second-line agents; newer drugs (bedaquiline, delamanid) under evaluation for extrapulmonary disease.
Follow-up: Endometrial curettage at 6 and 12 months; relapse reported in ≈ 22 % within 3 years. Despite microbiological cure, structural damage often persists.
Research & Future Directions
Novel diagnostics: Multiplex PCR panels, next-generation GeneXpert, cfDNA assays to improve sensitivity without sacrificing specificity.
Endometrial regeneration: Pilot studies on mesenchymal stem cells, platelet-rich plasma, nano-carriers, and growth-factor scaffolds aim to reverse intra-uterine adhesions.
Targeted therapeutics: Trials exploring shorter all-oral MDR regimens and immunomodulators (e.g., host-directed therapies) are ongoing.
Key Take-Home Messages
High index of suspicion is essential in women from endemic areas presenting with unexplained infertility or atypical menstrual disorders.
Combined diagnostic strategy (histology + molecular testing + imaging) maximises detection in this paucibacillary disease.
Early treatment yields excellent microbiological outcomes, but fertility restoration remains limited; prompt diagnosis before irreversible damage is crucial.
Advanced reproductive techniques offer hope but success hinges on preserved endometrial function—highlighting the need for continued research into regenerative therapies.
Selected References
Sharma JB. Genital tuberculosis in females. Int J Reprod Med. 2017:1–9.
Neonakis IK, et al. Female genital tuberculosis revisited. Eur J Clin Microbiol Infect Dis. 2020.
Schaefer G. Tuberculosis of the female genital tract. GLOWM; updated 2022.
⚠️ Disclaimer: This content is intended for educational purposes only and should not substitute professional medical advice, diagnosis, or treatment.
#Pathology #WomensHealth
#MedicalEducation #NotasDePatologia
#UterineTuberculosis #GenitalTuberculosis
#MedicalEducation #NotasDePatologia

English
Simin รีทวีตแล้ว
Simin รีทวีตแล้ว

Català
Simin รีทวีตแล้ว
Simin รีทวีตแล้ว

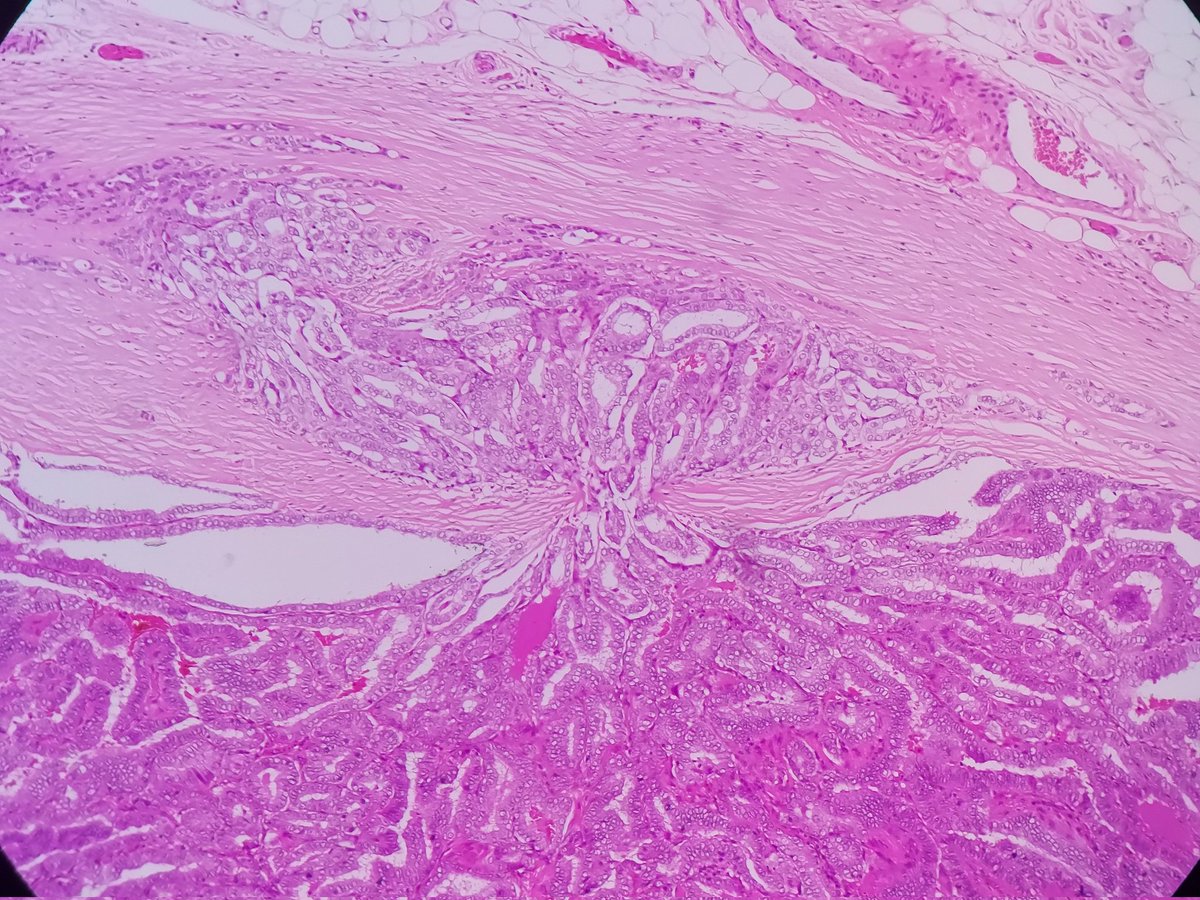
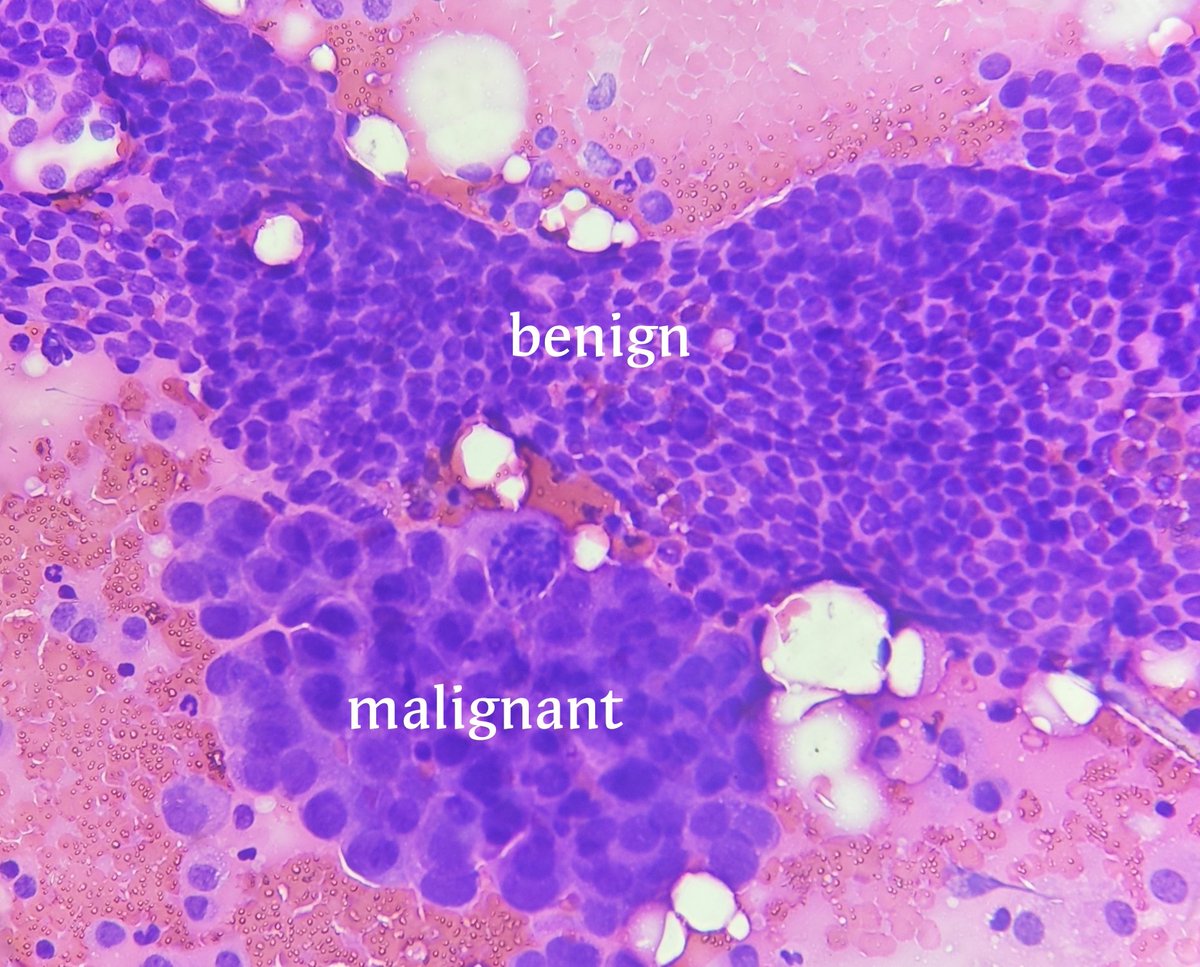
Breast lesion diagnosis ? See poll below 👇
#breastpath #pathresidents #pathtwitter #BreastPatholog1
@ColumbiaPath @Columbiapathre
@TheISBP

English
Simin รีทวีตแล้ว


English
Simin รีทวีตแล้ว

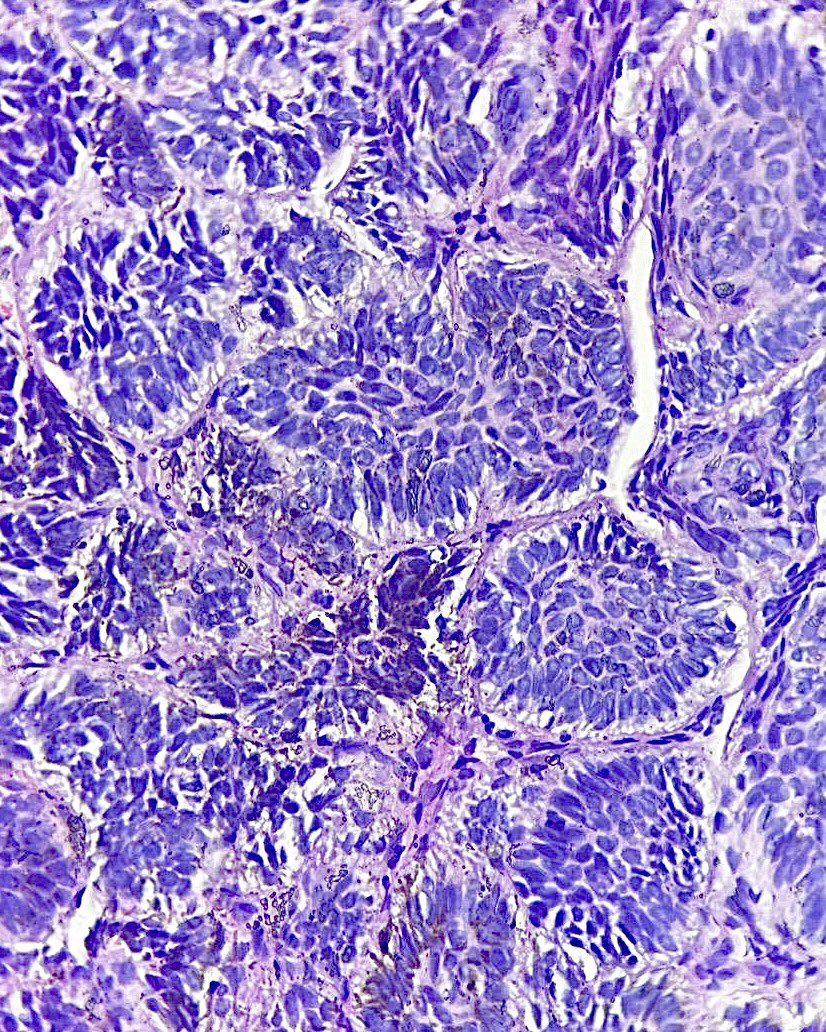
31 yrs old lady with right ovarian tumor. The gross and histologic patterns are consistent with stage IA dysgerminoma.
#pathology #gynepath #dysgerminoma




Myanmar 🇲🇲 English
Simin รีทวีตแล้ว


English
Simin รีทวีตแล้ว

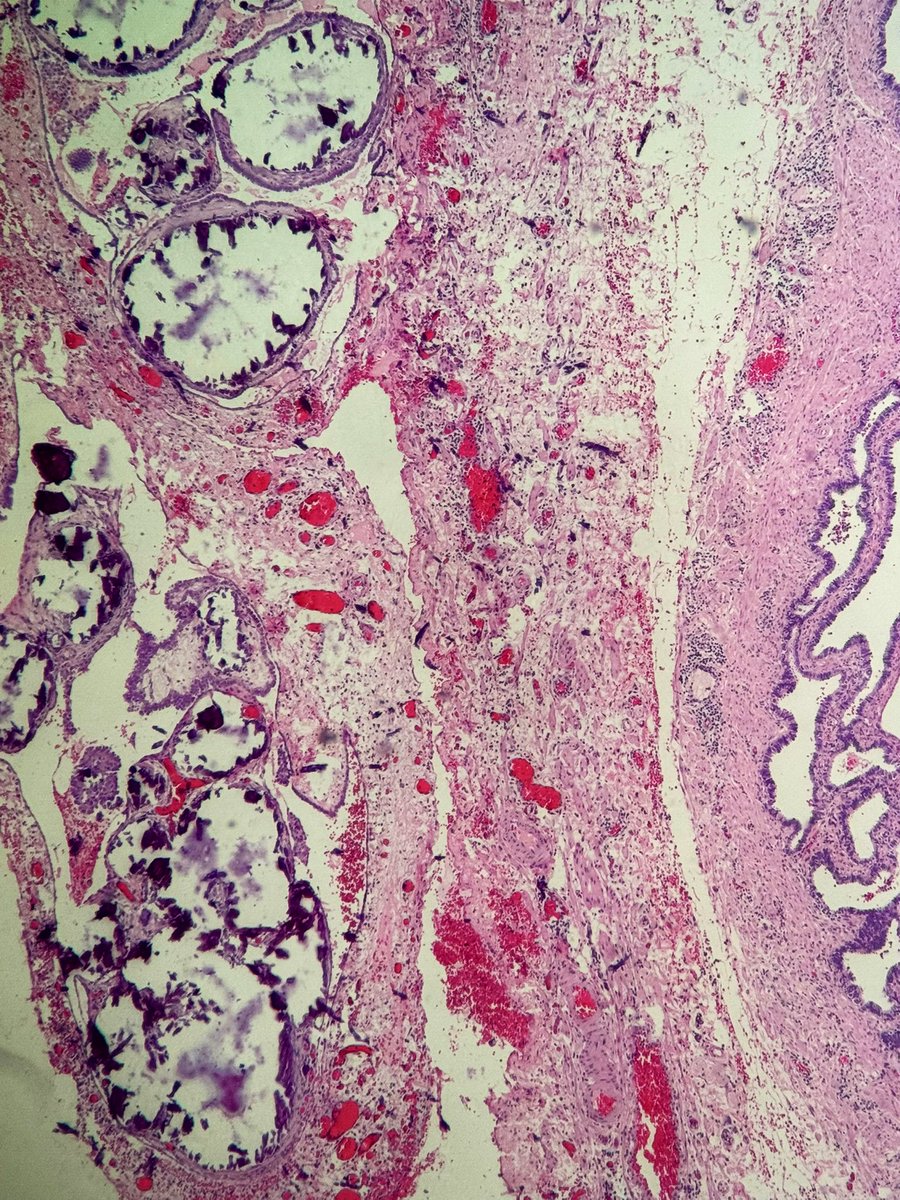
30-year-old woman with ectopic pregnancy. Incidental finding on the tubal surface. #gynpath #pathology

English

I MATCHED! I’m going to be a pathologist! 🔬🤓❤️
So grateful to my family, friends, mentors, and everyone who helped me get to where I am today. #FuturePathologist #MatchDay #PathMatch25 #Path2Path #Match2025 #Pathology #MedTwitter #pathX #pathmatch25

English


Today, I was honored to present our work titled “Enhancing Digital Pathology: Reducing Blurred Images of Immunohistochemistry Slides through Staining Protocol Optimization” @UTMB_Pathology at the 10th Annual Quality Improvement and Patient Safety Poster Session.



Galveston, TX 🇺🇸 English
Simin รีทวีตแล้ว

Ulcerative lesion over temporal lesion since 10 years!
#Dermpath
#pathology #pathology #PathX #Pathtwitter #SurgPath #Pathresidents

English
Simin รีทวีตแล้ว


Simin รีทวีตแล้ว

The post you've all been waiting for - introducing our amazing panels who will be answering all of your match questions this Saturday, April 12th!
@Anaisa_QA @Aberry_Med @cadaver_cami @AaronDobbins87
#Match2025 #PathMatch25 #PathMatch2025 #PathTwitter #PathX #Path2Path

English
Simin รีทวีตแล้ว

Skin biopsy. A pathology classic. One pic only.
Answer ✅ youtu.be/yfs42lmFZfU
#pathology #pathologists #pathTwitter #dermpath #dermatology #dermatologia #dermtwitter #usmle

YouTube

English
Simin รีทวีตแล้ว
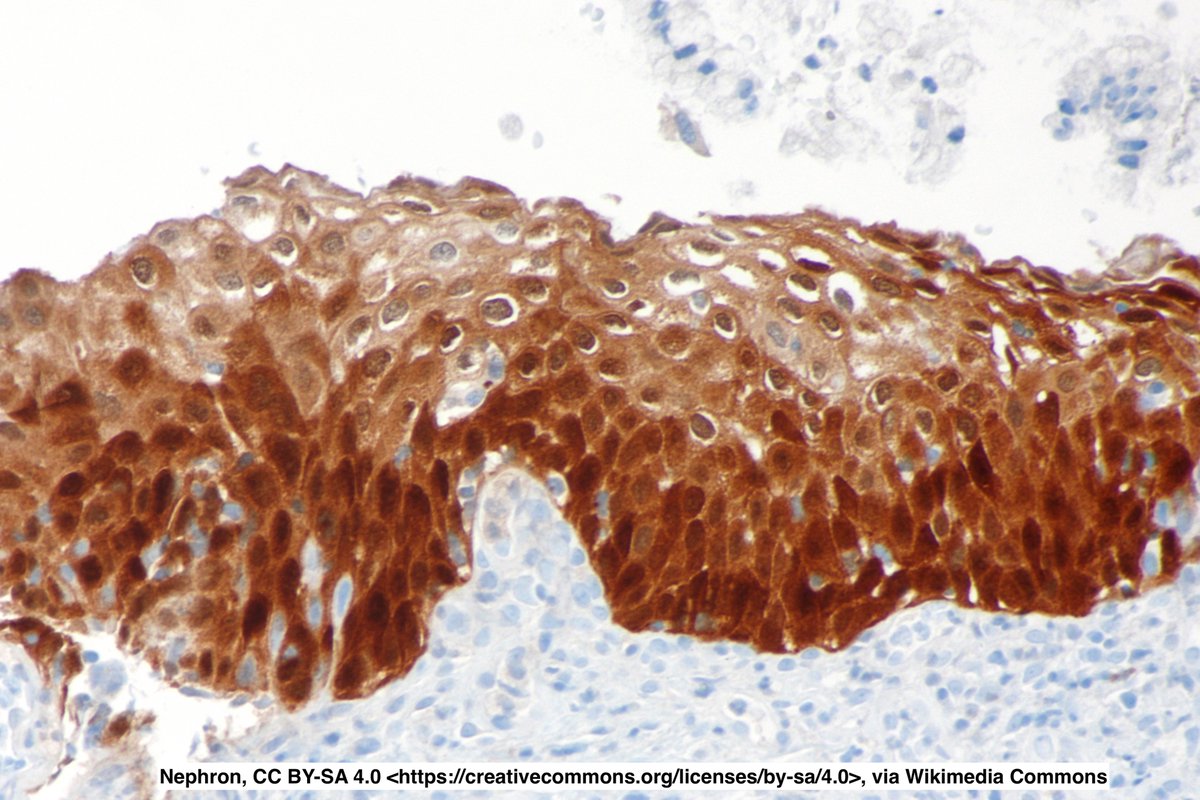
When I first started residency, I thought "oh p16 block +... HPV infection!💡"
Then I saw other non-HPV entities that were p16+ (eg liposarcoma)
p16=a surrogate for HPV infection:
E7 protein HPV -> inactivate RB -> p16 +++
But other tumors can also inactivate Rb -> p16+++
English