Tom Jayram รีทวีตแล้ว

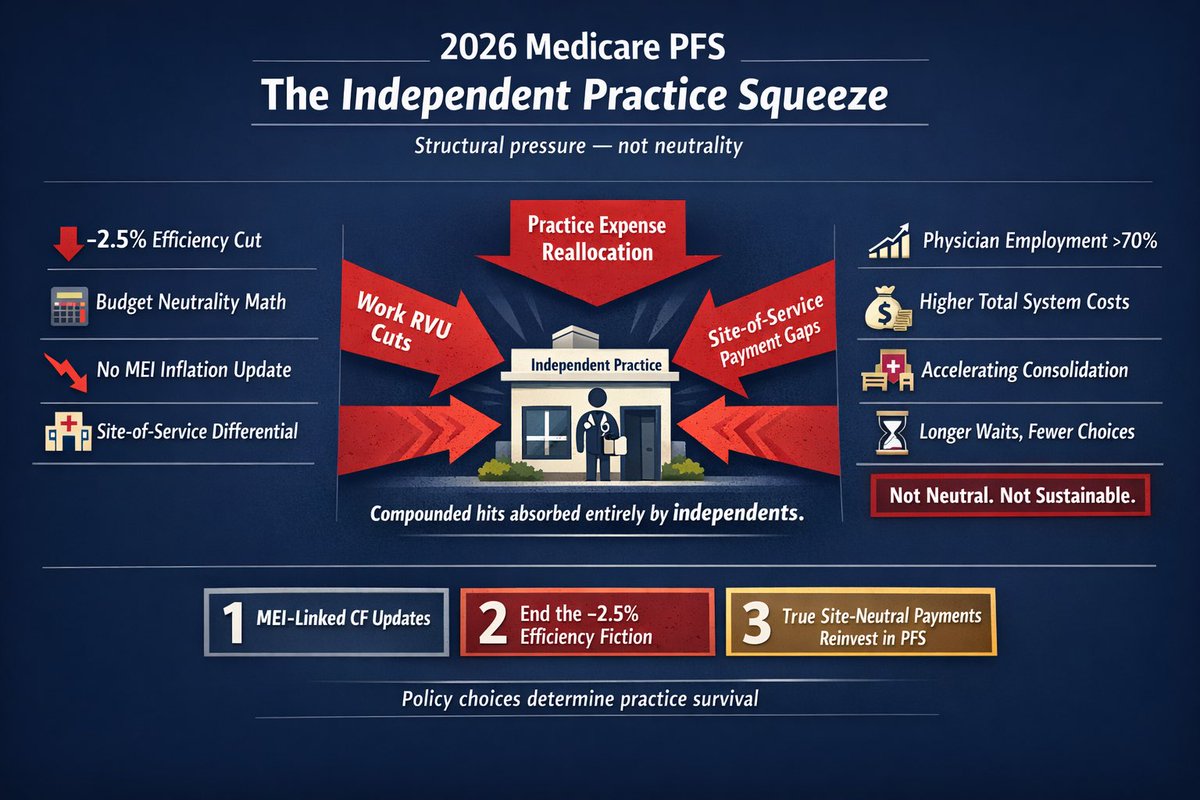
2026 Medicare Physician Fee Schedule: The Bottom Line — and the Fixes That Matter
After a full week dissecting the 2026 Medicare Physician Fee Schedule, one conclusion is unavoidable:
The PFS is no longer neutral. It structurally disadvantages independent, patient-centered care and accelerates consolidation.
Yesterday’s hearing suggest Members on both sides of the aisle understand how critical it is to reduce consolidation.
Here’s what the data show:
- The headline 3.26% conversion factor increase is temporary and misleading. There is still no permanent inflation adjustment, while a new –2.5% “efficiency” cut to work RVUs compounds pressure on physician payments.
- The efficiency adjustment itself is fundamentally flawed. It ignores rising patient complexity, double-counts prior optimization, contradicts operative time data, and disproportionately targets procedural services.
- Site-of-service distortions continue to widen. Identical outpatient services can be paid hundreds of dollars more in hospital outpatient departments than in physician offices, actively rewarding hospital acquisition and employment.
- Independent practices absorb the full weight of these changes — across work RVUs, practice expense, and site differentials — while employed physicians remain partially insulated.
The predictable result is that employment now exceeds 70%, competition erodes, patient access narrows, and total system costs rise.
Budget neutrality should not mean practice insolvency.
What Congress and CMS Must Do — Now
If policymakers want to preserve choice, competition, and access, the path forward is clear and bipartisan:
1. Establish permanent MEI-linked updates to the PFS
Indexing the conversion factor to the Medicare Economic Index provides baseline stability and prevents continued erosion. H.R. 6160, for instance, does exactly this and reflects recommendations from the medical societies, MedPAC, and the Medicare Trustees.
2. Repeal or overhaul the –2.5% efficiency adjustment
Across-the-board cuts based on assumptions (not service-specific data) distort care delivery. If repeal is not possible, any future efficiency adjustments should rely on empiric evidence, updated surveys, and transparent methodology.
3. Implement true site-neutral payment reform with reinvestment
Equivalent outpatient services should be paid equivalently, regardless of ownership. Closing site-of-service loopholes and reinvesting savings back into the PFS lowers costs for patients and taxpayers while stabilizing physician practices.
None of these reforms are radical. They are evidence-based, bipartisan, and widely supported.
The real question is timing.
Will policymakers act now or wait until independent practices have largely vanished?
The future of specialized, patient-first care depends on the answer.
English