
CardioTechx đã retweet
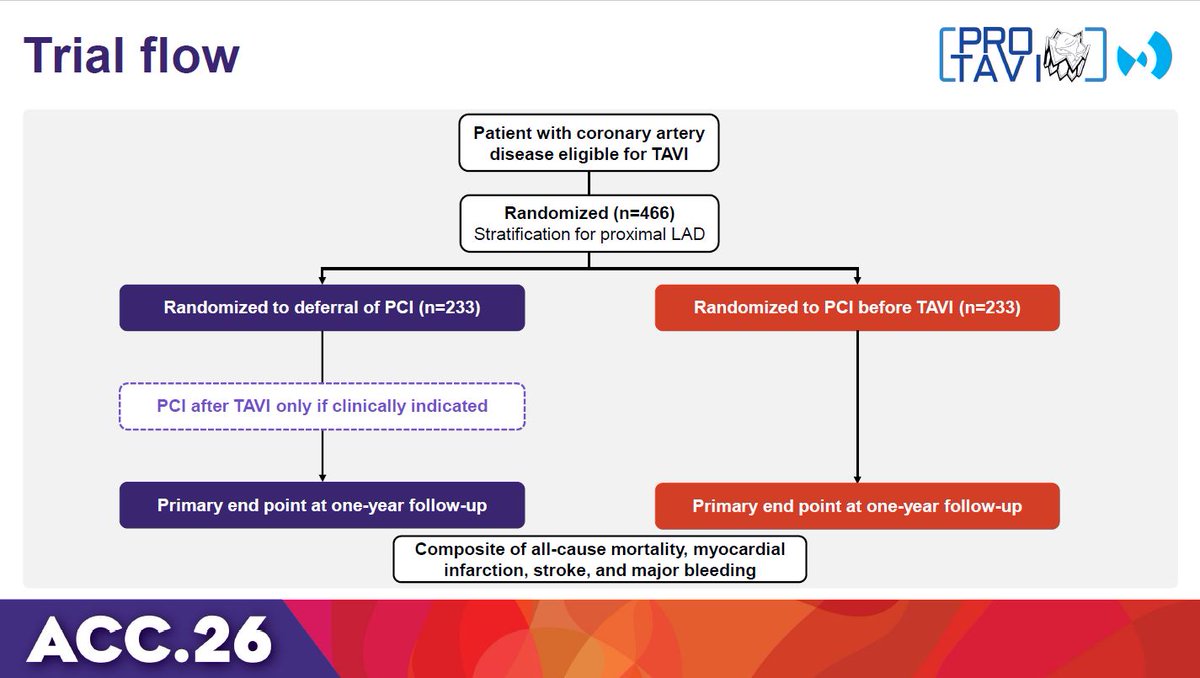
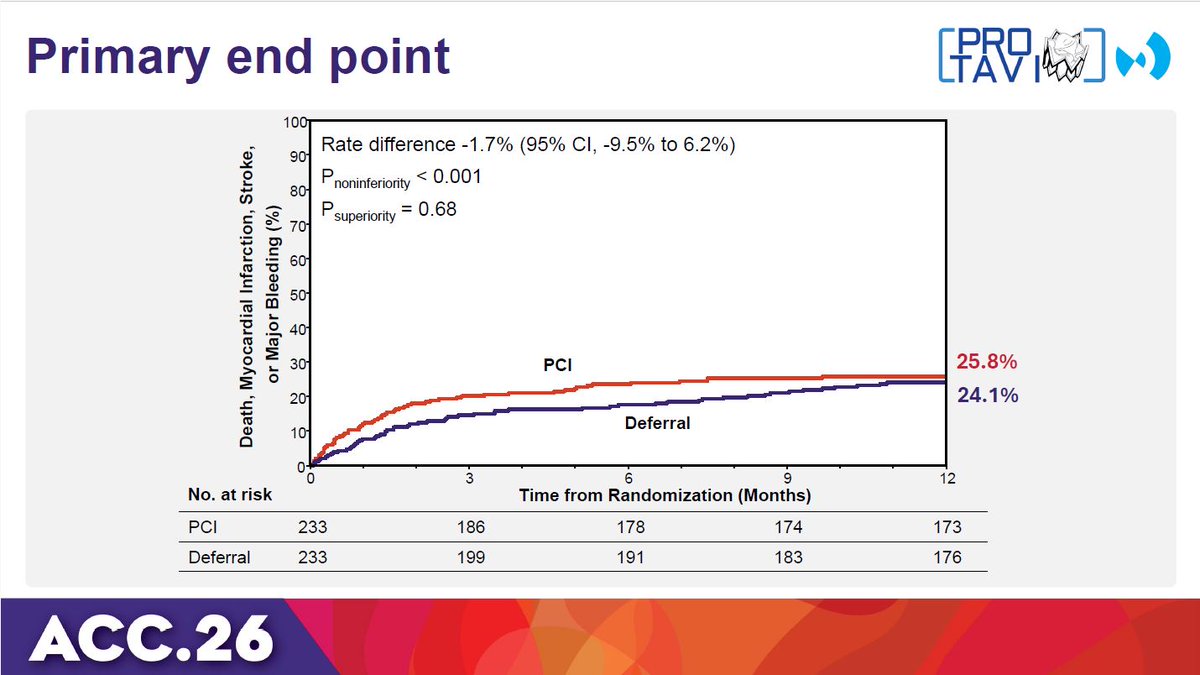
PRO-TAVI trial: Deferring PCI was non-inferior to routine PCI before TAVI for the 1-year composite of all-cause mortality, MI, stroke, and major bleeding, suggesting its appropriate role in selected CAD patients. #ACC26 View slides here: clinicaltrialresults.org/wp-content/upl…
English