
@Jakub_moscicki Filozoficznie, to my w sumie opisywaliśmy życie.
Wszyscy najbardziej lubili zawsze zadania tego typu 🤣🤣🤣

Polski
Tomasz Jetka
1.1K posts
@TJetka
Maths x Bio x Bioinf x Drug Development, PhD. Building AI x Bio in Poland.



Urodziny 🎂 w Brazylii, na ICLR 2026, prezentując na sesji nasze (Ingenix) rozwiązanie do modelowania zadań omicznych. W sumie w zeszłym roku trudno byłoby mi to zaplanować ☺️ (MLGenX) #icl2026 #ai #mlgenx

Simply retrieving a reasoning trace looks a lot like human reasoning, until it's time to navigate uncharted territory. If you memorized all reasoning traces of humans from 10,000 BC, you could automate their lives but you could not invent modern civilization.

very cool work. more dna language model pilled than i was an hour ago when i wrote my Evo 2 article a long time ago (owlposting.com/p/a-socratic-d…) the question was always 'how do you interpret the outputs of these models if it just spits out log-likelihoods?' and increasingly the answer is 'use probes to annotate embeddings, and ask the LLMs to interpret those'. in feb 2025, when i wrote my article, i didnt really trust the models to do that well. now i do, and perhaps there is an immense amount of greenspace for really crazy things to be done but one of the big failure modes of LLM-for-science approaches is that the models try really hard to be consistent with the data instead of reality. theres no experimental validation here, so who knows whether that's happening here id be extremely curious for someone to cross-reference the annotated VUS's here with, e.g. the UK Biobank 500k~ exomes with linked phenotype data. maybe Claude one-shot human variant function annotation, or maybe the annotations are slop, or maybe its in between



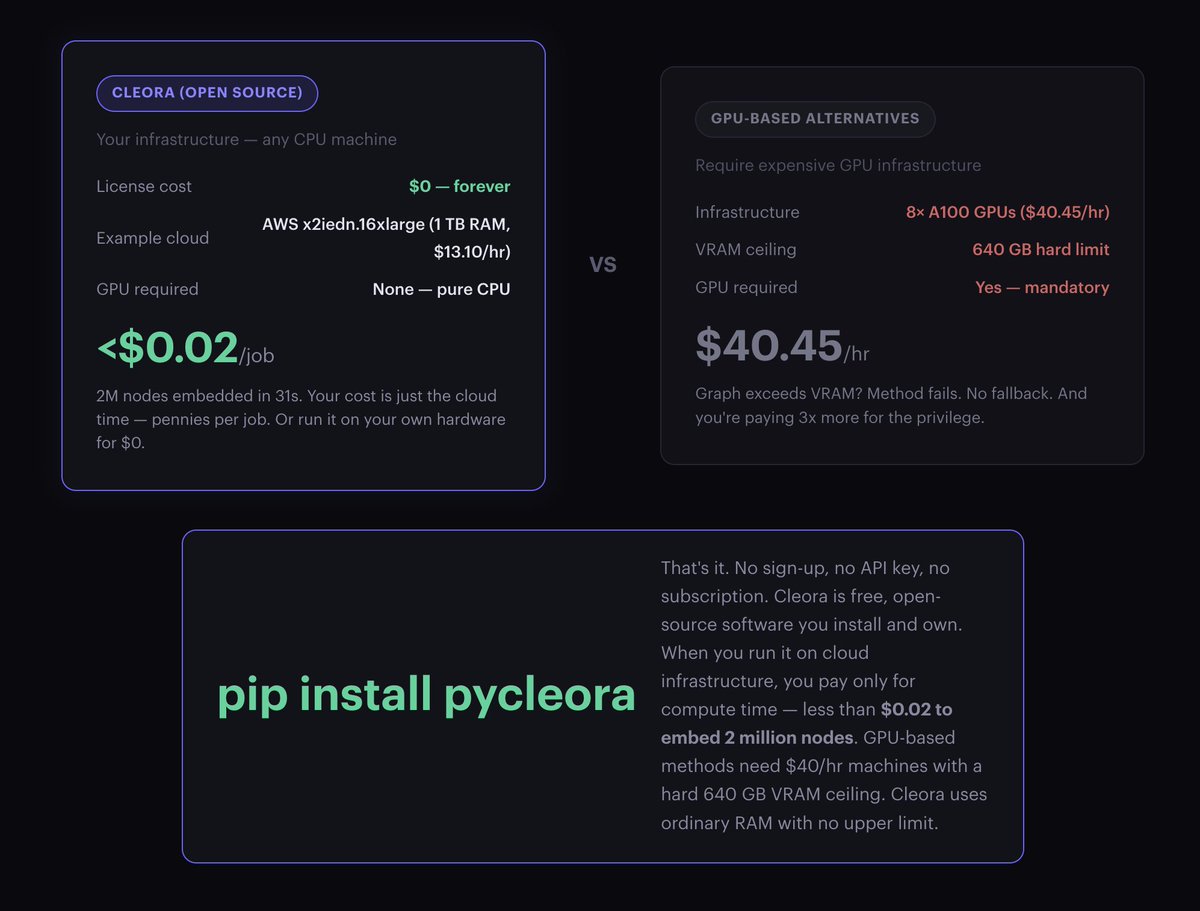

Prawie 7 lat temu, gdy hype na #ai był zdecydowanie mniejszy niż dziś, open-source’owaliśmy część naszego IP w obszarze #AI. Wówczas pokazaliśmy, jak wiele można osiągnąć dzięki doskonałości algorytmicznej. Dziś robimy kolejny krok. Publikujemy Cleora 3.2: Algorytm, który nie powinien istnieć ✨ Maksymalna dokładność. Polska 🇵🇱 technologia. cleora.ai Embedding grafu o 2 milionach węzłów w 31 sekund. Na jednym rdzeniu CPU. Za mniej niż $0.02. Bez GPU. Bez random walks. Bez negative sampling. 100% open source. Suwerenne AI to kontrola nad kodem, kosztami obliczeń oraz możliwość pełnej inspekcji i wdrożenia. Od zastosowań biomedycznych po analizę złożonych sieci - Cleora pozwala iterować w tempie, które wcześniej było nieosiągalne. Bravo @Synerise Research Team! #science #bigdata

Why do new buildings seem, on average, uglier than old buildings? We discuss some options: - Survivorship bias: only the beautiful old buildings have survived (we reject this option); - Cycles of taste: everyone always finds new buildings uglier (we mostly reject this too); - Ornament became too expensive because of rising labour costs (we reject this); - Ornament became too cheap because of mechanisation and then became low status (we reject this); - Some sort of Protestant or Puritan anti-beauty inheritance (we are doubtful); - Some kind of elite status game, perhaps a response to democratisation or elite overproduction (we think there is promise here, but serious work is needed on the details). I discuss this and more with @Aria_Babu and @bswud. Apple podcasts: podcasts.apple.com/gb/podcast/did… Spotify: open.spotify.com/episode/2pIka6… Youtube: youtube.com/watch?v=qvueKt…




Polska chciała postawić w Paryżu pomnik Józefa Poniatowskiego. Projekt był tak ważny, że rozmawiali o nim Donald Tusk, Andrzej Duda i francuski prezydent Emmanuel Macron. Rok później rzeźby wciąż nie ma, bo trzy polskie ministerstwa nie potrafiły ustalić, kto powinien zapłacić za jego budowę. A ambasador, który prowadził projekt, został odwołany z placówki w związku z aferą Collegium Humanum. zero.pl/news/nie-bedzi…

The story about bureaucracy almost stopping a man from treating his dog’s cancer with an mRNA vaccine went viral. The problem transfers to humans: we’ve made these clinical trials unnecessarily hard, denying hope to patients. New article on this. writingruxandrabio.com/p/the-bureaucr… Excerpts: "A story about Paul Conyngham, an AI entrepreneur from Sydney who treated his dog Rosie’s cancer with a personalized mRNA vaccine, has been circulating on X since yesterday. What makes the story inspiring is the initiative the owner showed: he used AI to teach himself about how a personalized vaccine could work, designed much of the process himself and approached top researchers to take it forward. Whether the treatment itself was fully curative and how much of an improvement it is over state-of-the art is not the main focus of this essay. Others have already debated that question at length, and I recommend following their discussions. What interests me instead is the bureaucratic absurdity the dog’s owner encountered while trying to pursue the treatment. He described the long and frustrating process required simply to test the drug in his dog: “The red tape was actually harder than the vaccine creation, and I was trying to get an Australian ethics approval and run a dog trial on Rosie. It took me three months, putting two hours aside every single night, just typing the 100 page document.” Even in a small and urgent case, where the owner was fully willing to fund the treatment himself, the effort was slowed by layers of procedure. Of course, this kind of red tape is not confined to Australia, nor to veterinary medicine. In fact, in the US, the red tape is even worse, at least for in-human trials. In a previous post, I recommended the Australian model for early stage In the United States, GitLab co-founder Sid Sijbrandij found himself in a similar position after the relapse of his osteosarcoma. When the ordinary doors of medicine closed, he entered what he called “founder mode on his cancer.” Like many entrepreneurs confronted with a difficult problem, he began trying to build his own path forward by self-funding his exploration of experimental therapies. Even then, he ran into the same maze of regulatory and institutional barriers that not only delayed him, but also unnecessarily raised the price of his experimental therapies. These are obstacles that only someone with extraordinary resources could hope to navigate, often by assembling an entire team to deal with them and navigate the opacity. In the end, Sijbrandij prevailed: he has been relapse free since 2025, after doctors had told me he was at the end of his options. Around the same time, writer Jake Seliger faced a similar situation while battling advanced throat cancer. Like Sid Sijbrandij, he was willing to try anything that might help. The difference was that Seliger was not a billionaire. He could not hire a team to navigate the system on his behalf, and he struggled even to enroll in the clinical trials that might have offered him a chance. A system originally conceived to safeguard patients has gradually produced a strange and troubling outcome: the mere chance of survival is effectively reserved for the very few who possess the means to assemble an army of experts capable of navigating its labyrinthine procedures. What makes these stories particularly frustrating is that we already know clinical trials — especially small, early-stage ones like the ones Sijbrandij enrolled in for himself— can be conducted far more cheaply and with far less bureaucracy than is currently required. Ironically, the original article cites Australia as a bad example, yet clinical trials there are conducted 2.5–3× cheaper and faster than in the U.S., at least for human trials, without any increase in safety events—a genuine free lunch. Removing unnecessary barriers has long been important. That is why I co-founded the Clinical Trial Abundance initiative in 2024, a policy effort aimed at increasing both the number and efficiency of in-human drug trials and have consistently argued about the importance of making this crucial but often neglected part of the drug discovery process more efficient. Since then, the issue has only become more urgent with the rise of AI. One of the central promises of the AI revolution is that it will accelerate medical progress. Organizations such as the OpenAI Foundation list curing disease as a core goal, and researchers like Dario Amodei of Anthropic have argued that AI could dramatically speed up biomedical innovation. But, as I have written before in response to an interview between Dario and Dwarkesh Patel, AI will not automatically accelerate a key bottleneck in making these dreams a reality: clinical trials. Conyngham’s observation that navigating the red tape to start a trial for his dog took longer than designing the drug itself only underscores the point. Clinical trials themselves vary widely. At one end are small, bespoke trials involving one or a few patients testing highly experimental therapies—like the treatment in the Australian dog story or the experimental therapy Sijbrandij pursued. At the other end are large-scale trials involving thousands of participants, designed to confirm earlier findings and support regulatory approval. Different types of trials require different reforms. In this essay, I will focus on the former: small, exploratory trials, which will be called early-stage small n trials for the purpose of this essay. These are often the fastest way to test promising ideas in humans and learn from them. They represent our best chance at a meaningful “right-to-try,” form the top of the funnel that generates proof-of-concept evidence, and may be the only viable path for personalized medicine and treatments for ultra-rare diseases. Understanding why these trials have been made unnecessarily difficult—and how we might change that—is essential if medical innovation is to keep pace with our growing ability to design new therapies. When the story first circulated on X, many people interpreted it as evidence that a cure already exists but simply hasn’t been used due to bureaucracy. That isn’t quite true, as I explained. The type of mRNA vaccine that the owner pursued looks promising, but he did not know a priori whether it worked or not, as it had not been tested before. So it was not a cure, but “a chance at a cure”. I hesitate to call it an “experimental treatment”, since this term evokes fears of potential safety issues while we generally can predict safety quite well now. The inaccuracy of whether this was a cure or not, however, does not make the story of the bureaucratic red tape that Conyngham encountered any less infuriating. More and more promising treatments are accumulating in the pipeline, fueled by an explosion of new therapeutic modalities, ranging from mRNA to better peptides and more recently, by AI. Yet we are not taking full advantage of them. To better understand these points, it is helpful to briefly outline the clinical development process—the sequence of in-human trials through which a promising scientific idea is gradually translated into a therapy. Drug development is often described as a funnel: many ideas enter at the top, but only a few become approved treatments. Early human studies, known as Phase I trials, sit at the entrance of this process. They involve small numbers of patients and are designed to quickly test whether a new therapy is safe and shows early signs of effectiveness. If the results look promising, the therapy moves to larger and more complex studies, including Phase III trials that enroll large numbers of patients to confirm whether the treatment truly works. Most people gain access to new therapies only after these large randomized trials are completed. On average, moving from a promising idea to Phase III results takes seven to ten years and costs roughly $1.2 billion. Accelerated approval pathways in areas such as cancer or rare diseases can shorten this timeline by relying on surrogate endpoints, but the process remains slow. As a result, many discoveries that make headlines today will take close to a decade before they become treatments that patients can widely access. Part of this delay is unavoidable. Observing how a drug affects the human body simply takes time. But much of it is not. Layers of unnecessary bureaucracy, regulatory opacity, and rising trial costs add years to the process without clearly improving patient safety, which is why I started Clinical Trial Abundance. Allowing a higher volume of small-n early stage trials, the focus of this essay, is a rare “win-win” for both public health and scientific progress. For patients, it transforms a terminal diagnosis from a closed door into a “chance at a cure,” providing legal, supervised access to cutting-edge medicine that currently sits idle in labs. For researchers and society, it unclogs the drug discovery funnel; by lowering the barrier to entry for new ideas, we ensure that the next generation of mRNA, peptide and AI-driven therapies are tested in humans years sooner, ultimately accelerating the arrival of universal cures for everyone. Next, I will explain why making it easier to run these early stage trials matters. First, from a patient perspective, they often provide the closest practical equivalent to a right-to-try. In theory, right-to-try laws allow patients with serious illnesses to access treatments that have not yet been confirmed in large randomized Phase III trials. In practice, these pathways rarely function as intended. Pharmaceutical companies are often reluctant to provide experimental drugs outside formal trials, and treatments typically must have already passed Phase I testing. As a result, very few patients gain access through these mechanisms. Early-stage trials offer a more workable alternative. They allow experimental therapies to be tested in structured clinical environments—often in academic settings or academia–industry collaborations—where patients can be monitored and meaningful data can be collected. Second, early-stage small-n trials are essential for personalized medicine and the treatment of ultra-rare diseases. Many emerging therapies—such as personalized cancer vaccines, gene therapies, and other individualized interventions—do not fit easily into the traditional model of large randomized trials involving thousands of participants. By their nature, these treatments target very small patient populations and often require flexible, adaptive clinical designs. From a societal perspective, these trials play a crucial learning role. As I argued in my earlier essay Clinic-in-the-Loop, early-stage trials are not simply regulatory checkpoints on the path to approval. They are part of the discovery process itself, creating a feedback loop between laboratory hypotheses and human biology. Later-stage studies, particularly Phase III trials, are designed mainly for validation: they test whether a treatment works under defined conditions and produce the evidence needed for approval. Early-stage trials, by contrast, are oriented toward learning. Conducted with small patient groups and often using exploratory designs, they allow researchers to observe how a therapy behaves in the human body and how the disease responds. In this way, they close the gap between theory and real-world biology. In the Clinic-in-the-Loop essay, I explain how these trials were crucial to the discovery of Kymriah, the first curative cell therapy for blood cancer."

This is false. RT-PCR of a gene-of-interest is an independent replicate. Even if the replicate is less accurate, it's still of value, since in many studies (e.g. scRNA-seq) there are no replicates at all (!) Of course ideally one designs good experiments from the outset.


