@JoseRestonVA @pawcio2009 On a side note Jose, are you back in Abivax? Or won’t be touching it for now?
English
Trading Doubled
127 posts
@TradingDoubles1
MSc Comp Sci, learning on the go


@pawcio2009 Did anyone have it in the Biopick?


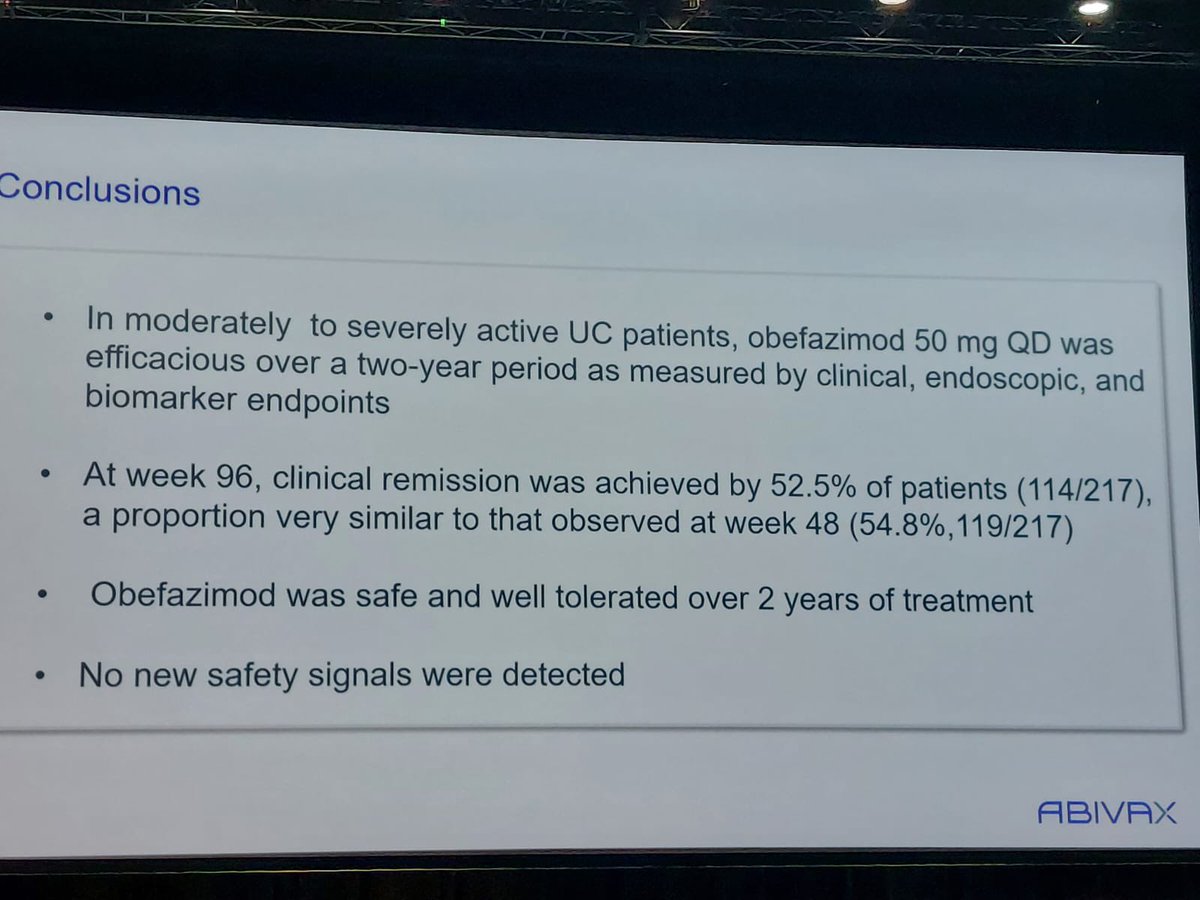
The IBD game has completely changed from symptom management (CR) to complete disease healing (ER). Now everyone will be forced to release ER. I don’t see CD failing with this kind of ER. I won’t be shocked if FDA also updates UC trial design & endpoint guidelines in future with emphasis on ER as important endpoint for approval. Patients love CR together ER over only getting CR while underlying disease is still there in bowel.






@grok conduct a Monte Carlo simulation to determine the likelihood that $ABVX would see a 7:1 imbalance in cancer cases between drug and pbo groups purely due to chance. Take into account background rates of cancer, as well as differences in time in treatment, age, pre-existing histories, and prior treatment histories between the two groups. Make no mistakes

@flippyfloppy52 unlike most on biox, i'm not blindly bullish on any stock, even ones i own and assets that i like. while i think $abvx obe efficacy is great, the malignancies will raise eyebrows among potential acquirers, given unknown moa. m&a value will likely dip below original assumption.

$ABVX Now that you have details from Abivax for each patient, see how 23 non-NMSC and 6 NMSC cases were reviewed for omvoh resulting in conclusion that not induced by the drug as the rate was still within the background rate for UC patients. Also, FDA review below.