PK
487 posts
PK
@PKCath
Interventional Cardiologist. hopeless healthcare for all advocate. average dude. opinions mine. RT not endorsement.
가입일 Aralık 2009
2K 팔로잉559 팔로워

I am recording my biggest video lesson yet:
"Financial Plan Presentation"
Showing how I walk through a comprehensive financial plan document, featuring 30 topic summaries.
If you'd like to see Susan and Steve Sampleton's entire financial plan for FREE, comment "Sample" here!
English
PK 리트윗함

Excited, scared, anxious, humbled, and beyond grateful to begin EP fellowship at @uazmedphx. Thanks to everyone who’s helped me to this point. But we didn’t come this far to only get this far. Time to get to work. Let’s go! @MikeZawanehMD @Peteweissmd @DrRoderickTung @su_wilber
English
PK 리트윗함

How is an 18yo allowed to buy 2 AR rifles & 375 rounds of ammunition when we wouldn’t let him buy a beer?
English
PK 리트윗함

These past two months I’ve realized my place is still on the field and not in the stands. That time will come. But it’s not now. I love my teammates, and I love my supportive family. They make it all possible. I’m coming back for my 23rd season in Tampa. Unfinished business LFG


English
PK 리트윗함

Starting July 22, second spot available for ACGME Acredited advanced heart failure & Tx fellowship.
2 fellows will have the finest balance of LVAD & Tx volume with 45 heart Tx & 40 LVADs annually. Contact me directly.
@KUMedCenter @KUHospital @KUMedicine @KUIMchiefs @KUMC_GME
English
@SVRaoMD @DrChuckSimonton @GreggWStone @JWMoses @MartyMleon @mmamas1973 @jason_wollmuth @rajivxgulati @DrMauricioCohen @KaulP @nolanjimradial Sunil - Thats the problem. Not a lot of trials but a good ultrasound/fluoro guided 4Fr femoral diagnostic cath probably has minimal risks comparable to radial if done correctly. Radial First doesn't have to be Femoral never. Would love any ref u have about 4Fr Fem vs 6f radial.
English

@DrChuckSimonton @GreggWStone @JWMoses @MartyMleon @mmamas1973 @jason_wollmuth What are the numerous trials comparing ultrasound guided femoral access with radial access showing similar outcomes? @rajivxgulati @DrMauricioCohen @KaulP @nolanjimradial
English

Try quick, easy ultrasound-guided femoral access with same risk profile based on numerous trials and save yourself radiation and time with no additional risk if patient has adequate femoral vessels. @GreggWStone @JWMoses @MartyMleon @mmamas1973 @jason_wollmuth
JM Schussler, MD@Updock
#Radialfirst people. You find yourself faced w a radial loop you cannot traverse. How often do you access ipsilateral #ulnarsecond ?
English
PK 리트윗함
PK 리트윗함

@mandeep_mayo Let’s remember indications for SIHD PCI (or perhaps ANY procedure in medicine). 1) Make the patient feel better 2) Improve the likelihood of living longer 3) prevent nonfatal events like MI, HF or VT. PCI can do 1, CAB 1+2, and GDMT all of the above.
English
PK 리트윗함

If anyone knows of an ICU bed for a C19+ patient who is in central Texas & in desperate need of dialysis please reply or DM contact info for the bed location & I'll pass along to pt's dr. Has tried 60+ hospitals already. Please amplify thx
English
@drjkahn @NIH @NIHDirector @Covid19Critical @PierreKory @stkirsch @BretWeinstein Joel - why are u peddling false info. The website states that there is insufficient evidence. NIH is not recommending anything. Please stop looking for twitter followers. Questioning the status quo is fine, but not at the cost of spreading misinformation.
English

Look what the @NIH @NIHDirector are recommending? The vitamins that @Covid19Critical recommended over a year ago! @PierreKory @stkirsch @BretWeinstein covid19treatmentguidelines.nih.gov/therapies/supp…
English
@Dr_Bitar @SFeitell I am sure this was a tough decision for all-not sure I agree with taking pt who is not in shock/angina free for high risk CTO and put in double LM stents for the belief that prog is improved - especially in this clinical setting. Good job though! Glad pt did well! Take care
English

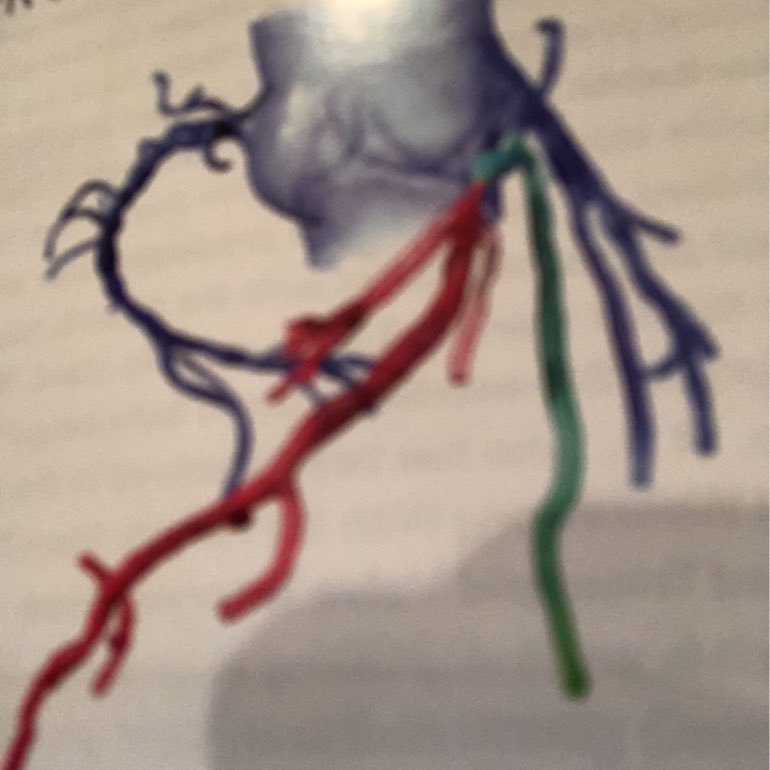
55 M Inferior STEMI at OSH, rx’d with PPCI developed CS requiring IABP then transferred @ROCRegional, EF 20-25%, small LV thrombus, pLAD CTO and distal LCx CTO. Smoker, metastatic 🫁 cancer with unresectable brain mets but prognosis > 1 y. CTS declined. Consult for CTO PCI.
Pittsford, NY 🇺🇸 English
Long discussion with patient and HF team lead by @SFeitell (So smart). Viable ♥️, BP with little room to start GDMT and antianginals. Ultimately agreed to procedure knowing this would be high risk. Waited until patient not requiring IABP (Impella not an option with LV thrombus).
Pittsford, NY 🇺🇸 English
@AndrewJSauer You can stop giving credit for ACE/ARB when 2/4 drugs you call pillars are as cheap as ACE-inh/ARB. Although we try to help patients thru prior auth, assistance programs and other measures, its definitely not cheap as $4 drugs for many. @JJheart_doc @AHajduczok
English

We cannot give credit for ACE/ARB anymore. I agree.
Fairway, KS 🇺🇸 English
@AndrewJSauer @DavidLBrownMD Also with increased risk of CABG upfront, why put someone who may not benefit from CABG, most of the benefit was not death but HF/CV hospitalization. May be with better drugs now, the trial would be null. So overall small # of pts ~100 and non-random viability testing. Thoughts?
English
I thought we learned from STICH to just revasc completely with CABG if targets and presentation appropriate and we learned viability imaging doesn’t help with decision making? @DavidLBrownMD
Diego Segura-Rodríguez@SeguraCardio
📌Myocardial Viability Before Surgical Revasc. in Ischemic Cardiomyopathy @JACCJournals #Review #TopicOfTheWeek #CardioEd #CardioTwitter #RadialFirst #EchoFirst
Kansas, USA 🇺🇸 English
@AndrewJSauer Not against new drugs or innovations but only 19% on ARNI, if trial had 75% on ARNI vs 19%, would we have seen the same benefit? I recognize that SGLTinh provide an alternative to pts who may be can't tolerate ARNI etc but so many drugs, so many co-pays. Trying to keep it simple.
English
PK 리트윗함

Until the joint commission has as much to say about safe staffing as they do about ice packs and writing on the doors of covid rooms and nurses drinking water, they should just stop wasting everyone's time and stay out of the hospital
English
@AndrewJSauer @JHMontfort10 @NavinKapur4 Andrew - I think you guys do great work but we need to stop wasting money on randomized trials of PA cath. Its a tool to obtain more information like a CXR, echo or any other test. Sometimes its obvious why a pt is in shock, other times I need more info. Use it prn.
English
So, a multi-center randomized trial enrolling HF-CS patients in the CICU to get PA catheter guided management vs care without RHC. Do we have equipoise to justify ethical enrollment? Also, would we achieve enrollment? - please address in comments. @JHMontfort10 @NavinKapur4
Overland Park, KS 🇺🇸 English
PK 리트윗함

After a week of arguing on social media with Anti-vaxxers and learning their arguments, this is how I think they’d run a hospital #covidvaccine #GetVaccinated #medtwitter
English