🚨PCR LBT🚨
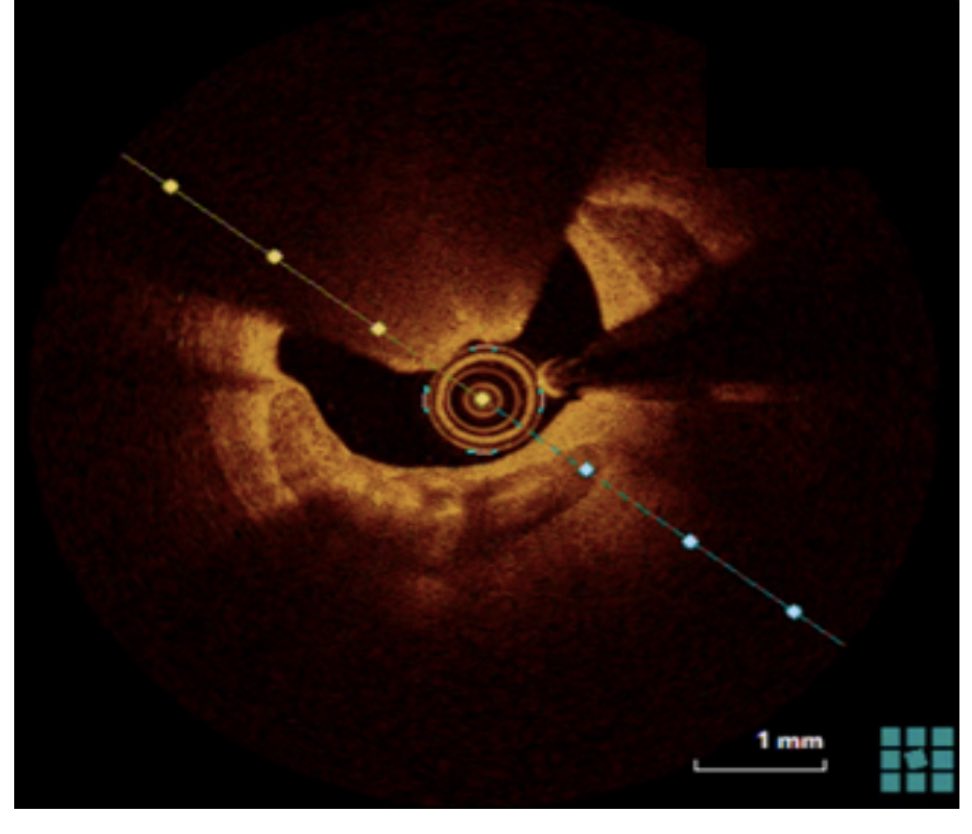
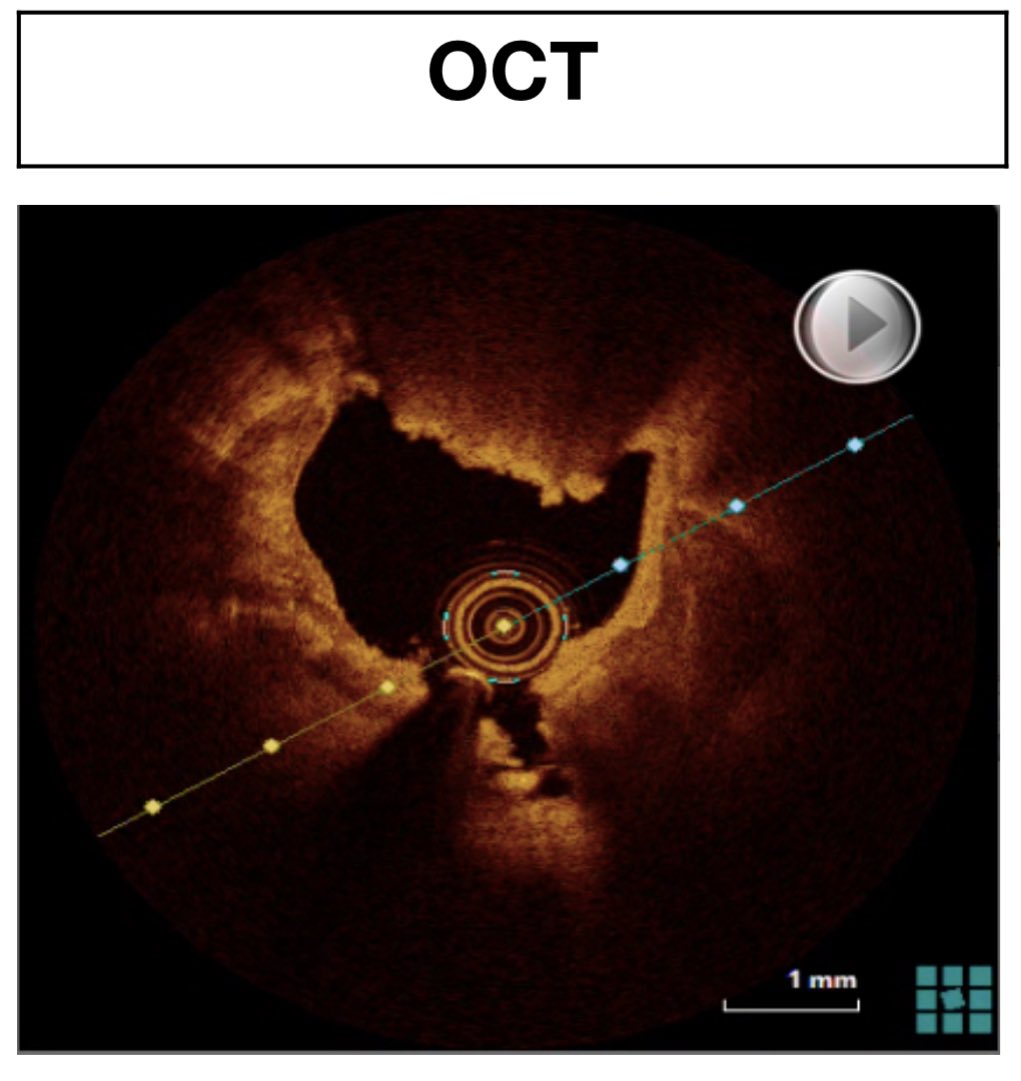
OCT-identified high-risk plaques in FFR-negative NC lesions associated with adverse longterm outcome after MI, with the difference predominantly being made on short term.
⚔️ attack HRP fast and aggressively for stabiliziation and risk mitigation?
@PCRonline
EuroIntervention@EuroInterventio
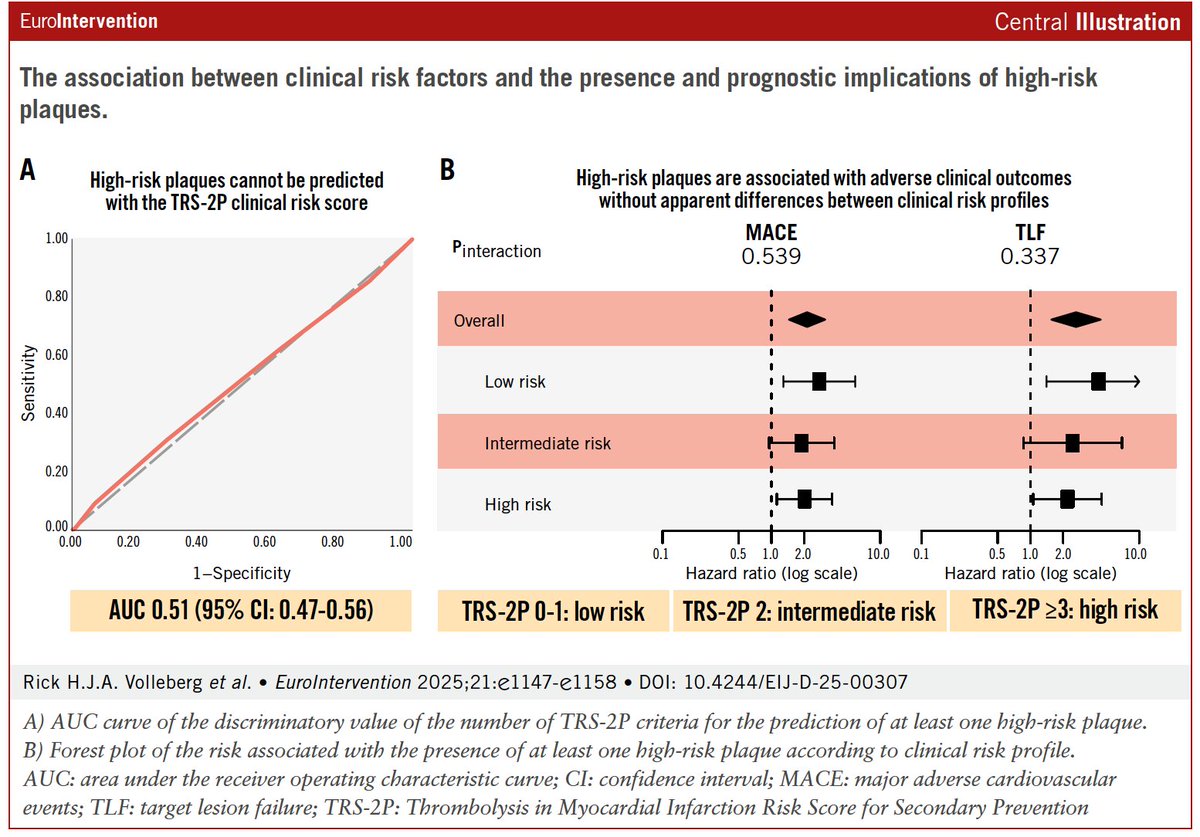
🔥 NOW ONLINE 🔥simultaneous presentation #EuroPCR PECTUS-OBS LONG TERM FOLLOW-UP In this study, OCT-identified high-risk non-culprit plaques with negative FFR were associated with a significantly higher risk of long-term adverse cardiovascular events after myocardial infarction. At 5 years, patients with at least one high-risk plaque had increased rates of non-fatal MI and unplanned revascularization despite non-flow limiting physiology. 🔗eurointervention.pcronline.com/article/long-t… @RickVolleberg @NielsRoyen @RGeuns
English