
Tristan Cordier
2.3K posts

Tristan Cordier
@SharkStats
Views are my own fleeting reactions. Statistics, Healthcare, Tennis, Soccer, Cooking, Family, Friends. We're all just atoms, bouncing around.
Washington, DC 가입일 Ocak 2010
1.1K 팔로잉308 팔로워

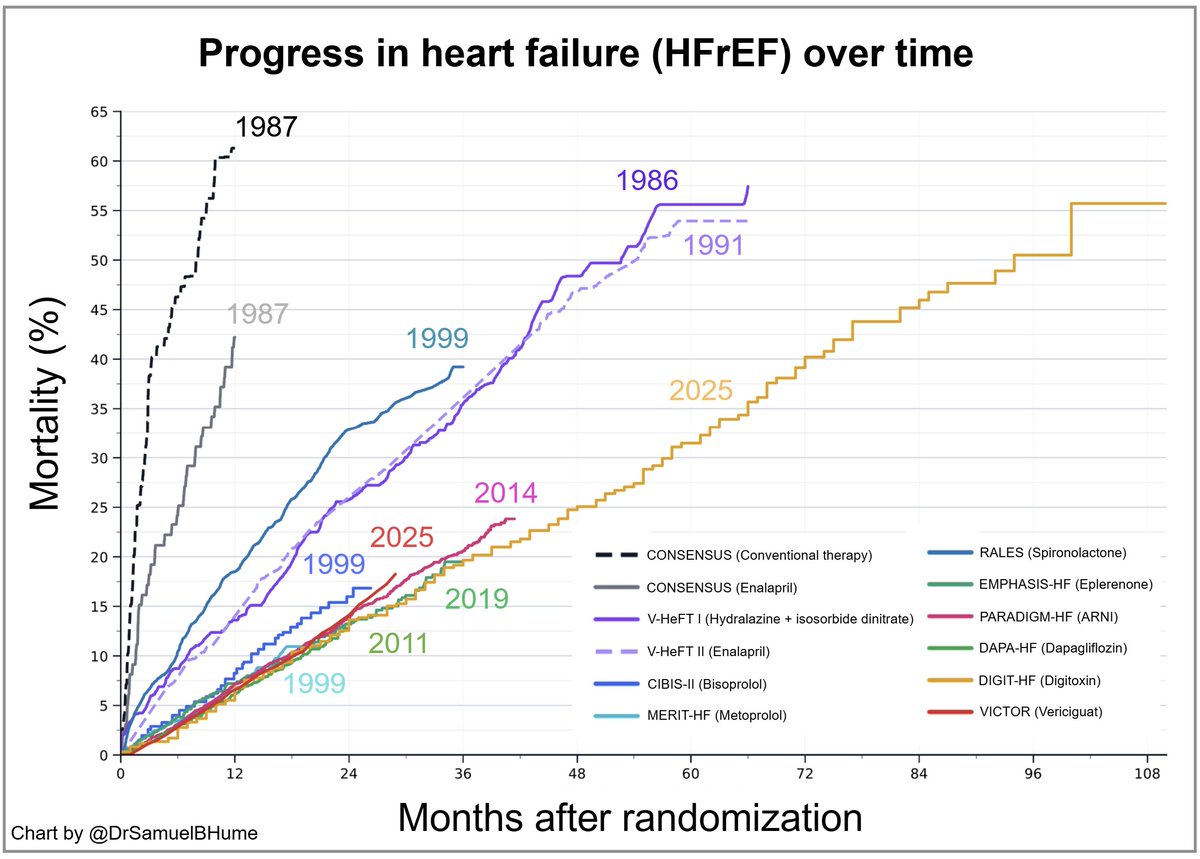
@DrSamuelBHume Neat! Thank you for building and sharing. Would be great to have a line for age standardized mortality as a referent point.
English


Nor should I. This is a very good idea even as it contravenes the way the law envisioned...
Elizabeth Warren@SenWarren
Elon Musk and Jeff Bezos shouldn't be paying the same amount in Social Security tax as someone making $175,000 a year. Billionaires are not paying their fair share.
English
@TheBorisBecker @atptour @DaniilMedwed @MattBerrettini Davenport beat Sharapova 0 and 0 at Indian Wells in 2005 when she was the reigning Wimbledon Champion and 3 seed.
English

Has anybody ranked as high as Medvedev ever lost a pro-match with a double bagel…
I mean 0:6 0:6 …@atptour ? @DaniilMedwed @MattBerrettini
José Morgado@josemorgado
Matteo Berrettini defeats world #10 Daniil Medvedev 6-0, 6-0 in 50 minutes to reach the last 16 in Monte-Carlo for a 3rd time. What the...
English
@RxRegA Thanks for speaking out during the saga. You put into words what many were feeling. Here is hoping the future FDA pursues high standards and US healthcare financing can slowly heal from lax oversight on this front.
English

Vinay Prasad’s exit from the FDA isn’t the “good riddance” story some media coverage has painted. In the wake of it, there’s real concern among many about what it means that someone with his background and approach to evidence standards wasn’t retained, and many came away from the media coverage of his tenure feeling cynically enlightened by it.
I saw him as a once-in-a-lifetime opportunity for FDA reform that was squandered. This isn’t fawning. I can admire someone and stay analytically grounded. This is about regulatory direction and evidence standards.
I wrote more about this earlier, and I still think it’s worth revisiting.
Jessica Adams@RxRegA
If you’ve been wondering why I can’t let go of the ousting of Vinay Prasad from the FDA, here it is, plain and unvarnished. He was a once in a lifetime hire. Prasad was one of the strongest appointments the agency has ever made, and the FDA should have fought like hell to keep him. That doesn’t mean I agreed with every call. For example, I support advisory committees. But it’s worth noting that advisory committees were already in decline prior to his appointment. Besides, disagreement with one aspect does not negate the whole. The failure to retain Prasad was a consequential mistake; it signals exactly how the agency, the media, and the investor class handle serious challenges to the status quo. And the backdrop makes it worse. Prasad walked into the CBER director’s office after a truly rough stretch in FDA history: overly broad use of COVID vaccines, with related resignations of two top vaccine officials, Paxlovid cheerleading, Elevidys and Aduhelm debacles, and misguided misinformation-policing, among others. This stretch had eroded public trust. He inherited a scarred institution, and the expectation was that he would challenge the status quo and repair the perception of the FDA as acting merely as a rubber stamp. What’s been maddening to watch is the yawning gap between what everyone claims to want, like higher evidence standards, fewer weak approvals, more appropriate use of accelerated approval, and how violently the system recoils the moment someone tries to deliver it. Modest, data driven moves were treated like heresy. The loudest critics rarely engaged the substance; they only amplified an outrage coming squarely from the perspective of pharma and investor interests. A clearer accounting of what actually changed and what didn’t during the time Vinay Prasad was at the FDA is still worth laying out. Accomplishments included the COVID vaccine framework, the Elevidys label narrowing, and proposing to strengthen CBER research and vaccine standards more generally. The Moderna flu vaccine refuse to file decision was an example of using an unconventional approach. It was resolved quickly in a manner that will result in better evidence generation, but with much media fanfare. And worth noting: not all of his accomplishments were around tightening standards. He co-authored significant approaches to introduce regulatory flexibility and support true innovation: formal guidance documents for the new plausible mechanism pathway and Bayesian methodology. Both of these are being praised, but no one is bothered that a key architect on these projects is leaving the FDA? Not to mention the single trial paper. Instead, the public narrative chose to fixate on three leadership overrides, endlessly framed as “chaos” or a break from sacred norms. Conveniently omitted: every single override aligned decisions with the new COVID vaccine framework that Prasad had developed to navigate uncertainty without rubber stamping. Approval volume stayed roughly in line with historical norms. Rare disease decisions weren’t some override spree; they were part of long running debates over accelerated approval pathways that predate Prasad by years. Reasonable people can quarrel over individual calls. What’s indefensible is pretending the record was defined by recklessness rather than a short, intense effort to tighten standards in an agency long accused of being too cozy with industry. ...
English
@itslennyj @CataPaul2 @SpecialSitsNews You're missing something. What happens when one nation's demand isn't met from oil flowing through one specific channel?
English

⛽️ Countries Most Dependent on Oil via the Strait of Hormuz
🇯🇵 Japan — 73%
🇰🇷 South Korea — 70%
🇮🇳 India — 42%
🇨🇳 China — 40–45%
🇵🇰 Pakistan — 60%
🇹🇼 Taiwan — 60%
🇹🇭 Thailand — 30–35%
🇸🇬 Singapore — 30%
🇲🇾 Malaysia — 25–30%
🇵🇭 Philippines — 25%
🇮🇩 Indonesia — 20–25%
🇻🇳 Vietnam — 20%
🇮🇹 Italy — 15%
🇪🇸 Spain — 12–15%
🇺🇸 United States — 2–5%

English


@viatoCEO Is your point that the goalposts have moved or that the drug is effective?
It may be dispiriting for those involved, but we cannot lean on past guidance to justify poor decisions. Think about what that means at a scale far beyond a single drug.
English

@SharkStats They developed this entire statistical analysis plan under FDA guidance.
They would have started a phase 3 long ago if the FDA didn’t lead them to believe this data was sufficient data to support a BLA.
Don’t act like the company is trying to “pull a fast one”
English

Tristan (@SharkStats ) is on target.
Approving a $3million/pop gene therapy drug that requires drilling into the skull and a brain injection should be based on... checks notes... a propensity score matched historical control arm. (If you can't appreciate the insanity of this sentence, you should comment zero times about science and evidence)
That is exactly what the biotech/investor community who cares so much about Huntington's disease patients would base approval on.
And then comes the surrogate data. It takes a few minutes of reading to understand how incredibly flimsy that is in the case of Huntington's disease.
The Roche/Genentech product tominersen you haven't heard of that failed was also very promising because it decreased a key surrogate biomarker: mutant huntingtin (mHTT) levels in CSF. But when the Phase III GENERATION HD1 trial ran, lowering mHTT didn't translate to clinical benefit.
The failure was particularly alarming precisely because tominersen did lower mutant huntingtin levels — the surrogate worked — but patients didn't benefit clinically. In fact, patients receiving the drug more frequently actually did worse than placebo.
From the GENERATION HD1 data:
The every-8-week group (higher exposure) showed:
cUHDRS scores significantly worse than placebo (–0.54 points, p=0.001) — this is a composite of cognition, motor function, and functional capacity, trends toward worse Total Functional Capacity (TFC) scores, and elevated CSF NfL at week 21 — suggesting active neuroaxonal damage was occurring.
So now since we can't use mHTT as a surrogate -- we have another unvalidated surrogate --
NfL (neurofilament light chain) is a marker of neuroaxonal damage/neurodegeneration. It's validated as a marker of injury, meaning it rises when neurons are damaged, correlates with disease severity and progression rate across multiple neurodegenerative diseases (HD, MS, ALS, Alzheimer's), and tracks with known disease milestones
But same issue with mHTT : it's validated against disease activity, not against treatment response leading to clinical outcomes. So we know high NfL = more neurodegeneration, we know NfL falls with some treatments, but we have zero robust proof that drug-induced NfL reduction → clinical benefit.
So of course we should get excited about nFL changes and scream bloody murder when someone asks to actually do an RCT to make sure we aren't hurting people, and are paying for something that actually has benefit.
English
@viatoCEO Statistical significance is not a cape to be draped over the shoulders of a poor comparison. If you read the points against your current perspective on this dispassionately you may come to appreciate that.
English
@anish_koka @SharkStats AMT-130 clinical benefit is statistically significant and supported by reduction in Neurofilament light.
There’s zero reason to shut the door on 4yr data which is due in 3-6 months.
If that looks good, accelerated approval with confirmatory RCT should absolutely be on the table
English
@IamnotDescartes @Macro_First Prior FDA regimes gave us high cost drugs with little to no efficacy. Those drugs are all baked into clinical practice and our healthcare costs today creating financial toxicity and potentially additional side effects to manage for patients. Biotech suffers today for future gain.
English

@Macro_First You’re totally right. The FDA is coming apart at the seams and their lack of regulatory clarity makes biotech uninvestable.
English
Usually, when senior FDA officials make scathing public comments like this about a biotech stock, the stock drops immediately by 30% or more. $QURE is actually up 15% today, which suggests the FDA's communication may be losing credibility.
CNBC@CNBC
FDA official calls UniQure's gene therapy a 'failed' treatment for Huntington's disease cnbc.com/2026/03/05/fda…
English
@crypto_pillz @anish_koka Wow. Propensity matched. It must be good. 🙄
English

@anish_koka Listen bozo…it was propensity score matched with Enroll-HD which is the largest global observational study and natural history dataset for Huntington’s disease, with over 30,000 patients tracked over many years.
English
The UniQure/FDA Huntington's gene therapy controversy explained :
1/ UniQure is battling the FDA in the press over a placebo-controlled trial requirement for their Huntington's gene therapy. Here's a brief summary. 🧵
English
@greta @HeathVeuleman Good point we should call them Medicals.
English

When did doctors become “health care providers?” Do they go to “provider school” now and not “medical school?”
English
@drkeithsiau Nooooooo I loved you when it was case studies. Please don't push retrospective observational trash.
English


@AnilMakam My god. A reasonable take and an acknowledgment that institutions are made up of people.
English

I read the NEJM piece carefully and read Vinay's previous paper on the same topic (screenshots in thread)
Moves from strict adherence to 1-2 RCTs toward a more context-sensitive position (because once in the shoes of the regulator different perspectives to now consider?)
What I like:
Still maintains a high evidentiary standard for trials, which we often did not see before (ie surrogacy, bad controls)
Retains flexibility to ensure a 2nd trial if first one sucks or is unclear
What I (really) don't like:
Creates a framework that works best under a regulator with higher evidentiary bar since a lot of this is in the eye of the beholder. So yes if Vinay, but slippery slope if Peter Marks (or any other past predecessor). That worries me since gives more wiggle room to lower the bar
Zach Brennan@ZacharyBrennan
FDA formalizes its shift to requiring only one pivotal trial (via NEJM) and analysts are already pointing at companies this could help -- another pro-pharma push for Makary, and another 180 for Prasad who wrote extensively in his academic life against trials focusing on anything less than overall survival endpoints.news/fda-formalizes…
English
@cremieuxrecueil Or people who tap out after Master's (doctors, lawyers, etc.) have higher IQ than those who proceed beyond that point. So not about grit but more about selection dynamics?
English

Reminder:
The genetic correlation between finishing a PhD and intelligence is lower than the genetic correlation between finishing earlier levels of higher education and intelligence.
The PhD ends up being more about gumption.
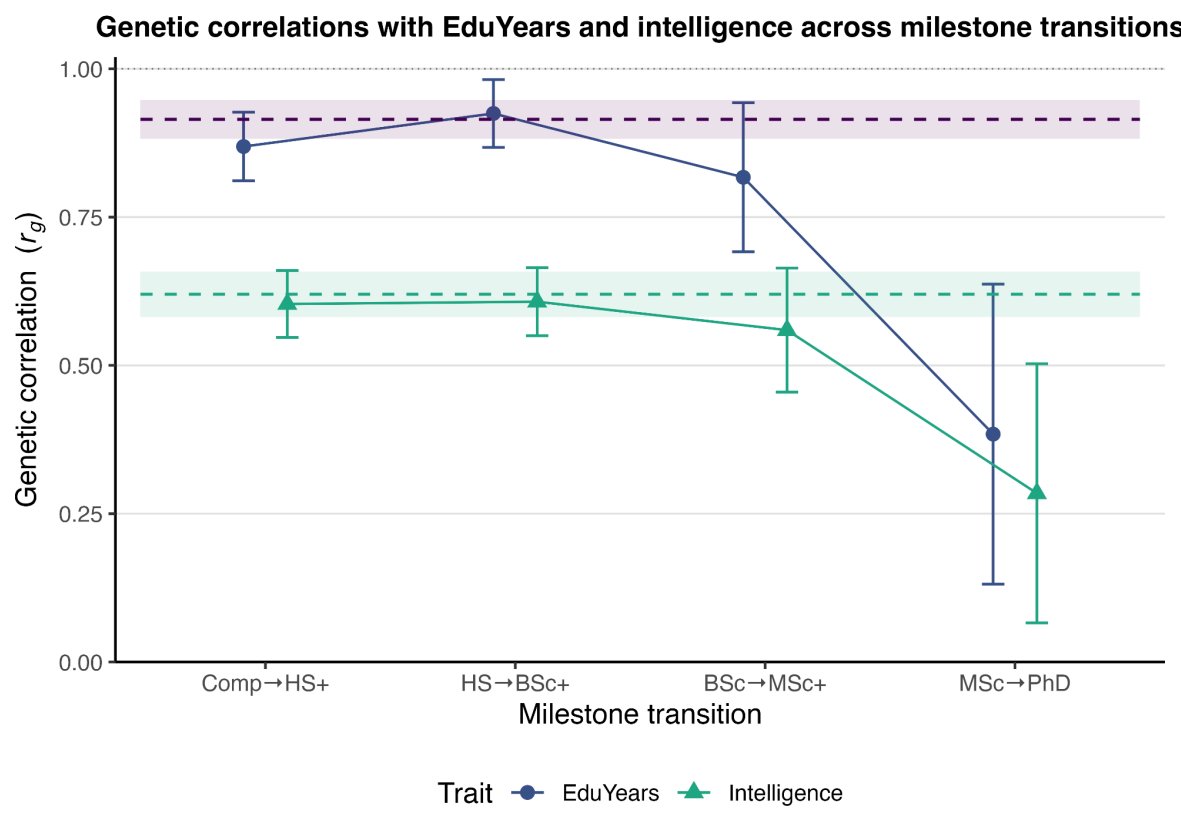
Crémieux@cremieuxrecueil
Educational attainment is a garbage phenotype: what it measures varies radically over time, types of education, and so on. As it turns out, once you get to the PhD level, its meaning radically drifts. Earning a PhD is less about intelligence or earlier EA than other EA levels:
English
@Forever_DNA @l_e_whyte Good point. We should value the needs of the biopharma sector which at no point in history has required reining in.
English

@l_e_whyte VP what an egotistical loser. he's hurting biopharma sector badly & sounds incompetent, entitled and totally just not worth it. Makary & RFK pleaded for him to come back; clearly shows their science chops & character flaws. It's a Podcast Bro Clown show @ the new FDA
English

WASHINGTON—In an hour-long meeting in January, Food and Drug Administration career staff laid out their objections to a plan to block a new flu shot from vaccine maker Moderna...
Vinay Prasad, the head of the FDA vaccine and biologics division, overruled them...
English
@nociFTW @RxRegA @AppleHelix Fair point but the signal/shock may also be a part of the point here. Lest you get Moderna'd, best get that control group right. Explosion in Medicare Part B and Part D costs is not helped by me too/ineffective agents being approved on weak evidence.
English
@RxRegA @AppleHelix I’m not sure. If you want to change standards, that’s ok, but then you do that FOR Future sponsors/trials. Not retroactively. It’s not legally secure.
English
What’s striking in this Moderna debate is how quickly arguments about evidentiary standards get reframed as hostility to innovation or vaccines. Disagreement about what evidence is sufficient isn’t the same thing as opposition to products.
English
@CNviolations We should all hope to be measured publicly by our worst moments.
English
How an ex-wife comes to pick up her kids from husband..
English
@W1ll0fTheP30ple @heresyfinancial And even to some without those wonderful faculties.
English

@SharkStats @heresyfinancial This is obvious to those with functioning brains and critical thinking skills.
English

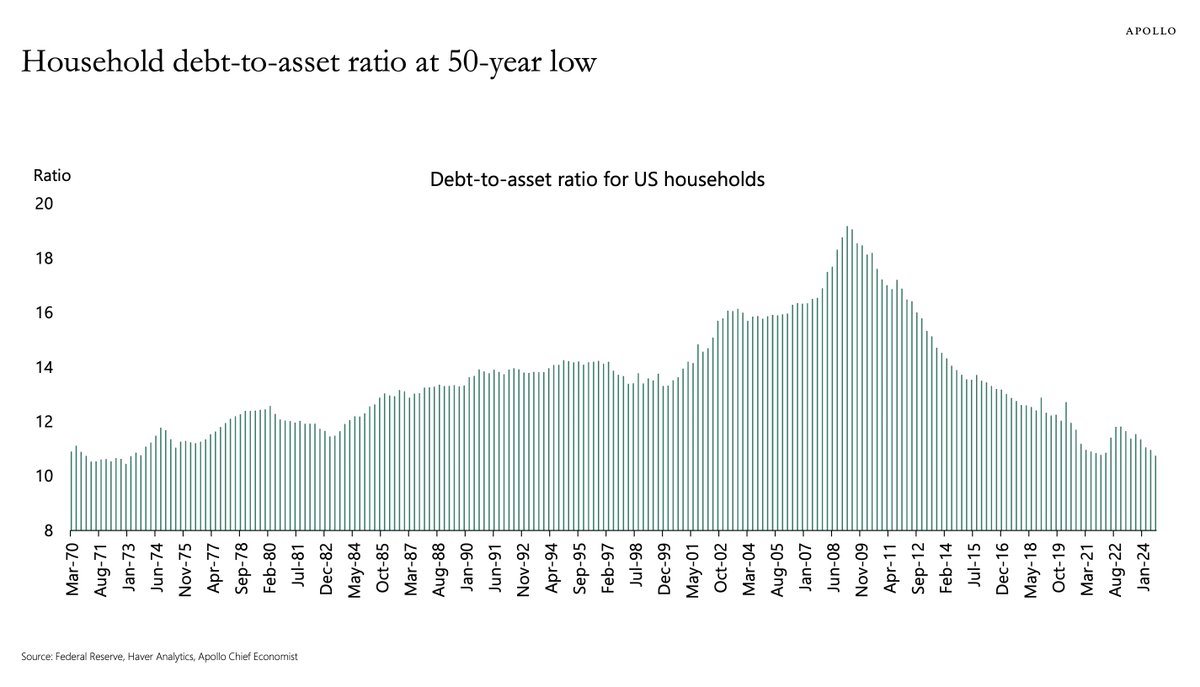
The US household debt-to-asset ratio is at a 50 year low
English