
Mohamed Ekshame
301 posts

Mohamed Ekshame
@ekshame
Orthopaedic Surgeon, special interest in sport medicine , gym and fitness addict , volleyball 🏐player
Libya 가입일 Ağustos 2014
1.6K 팔로잉297 팔로워

@traumaticum Short working length of plate, too many distal screws will add to destruct vascularity of the already poor biology
English

why did this go onto non union?
60yo F, moderate energy trauma. Methotrexate and Secukinumab. Index LISS OP 10m ago
Im expecting 1000's opinions, so have created a poll to capture the vibe⬇️
feel free to add more detail in the comments
#orthotwitter
#orthopedics
#orthopaedics


English

Meniscus Monday!
How would you repair this torn meniscus? (Hint: the picture shows a useful tool)

English
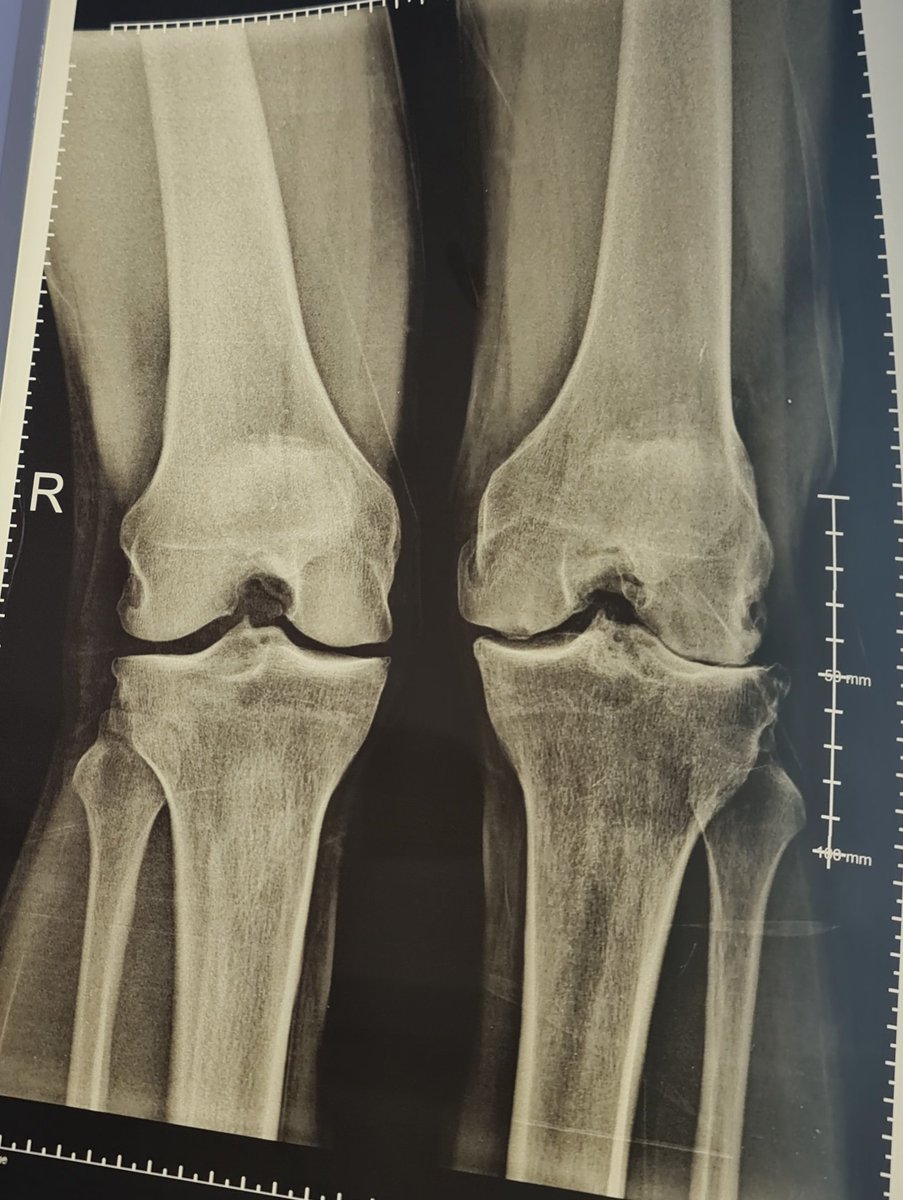
@hjluks 49 M , lt knee menisectomy 2002 and ACL tear , mild pain after Sport , when I examined the right knee I found it even more unstable than left but no complain! , so
Bilateral ACL tear , menistomy in left knee and still running, playing football in age of 49
Libya 🇱🇾 English

Love these cases.
This 50 something is running, swimming and cycling.
Running the Brooklyn Half in May.
Gotta love it
With permission.


English


@neiljainortho @TheISEH I would like to join Bostaa , but they asked for proposer email , if you can help , thanks in advance
English

Pleasure to be at #BOSTAA Annual Conference for a day of Instability in Sport! @TheISEH #sportstrauma #arthroscopy

English


@DrNikhilVerma I only use pump for ACLs and hip scopes, gravity for all others. What are your pump pearls? Do they vary by joint? What are some potential pitfalls? I think a lot of attendings and residents could benefit from this.😃
English

Triple digits on the pump!
Your pump is your friend— you can push it hard if you move expeditiously!

English
In many cases meniscocapsular separations are hidden unless you dislocate them, inside out set with our magic reuseable needle is a cost effective and can save your patient’s knee
#arthroscopy #savethemeniscus #sportinjuries
English

ACL reconstruction 1 year ago. Still don’t get why it failed 🤔
I would ban that surgeon from surgery if I could


English
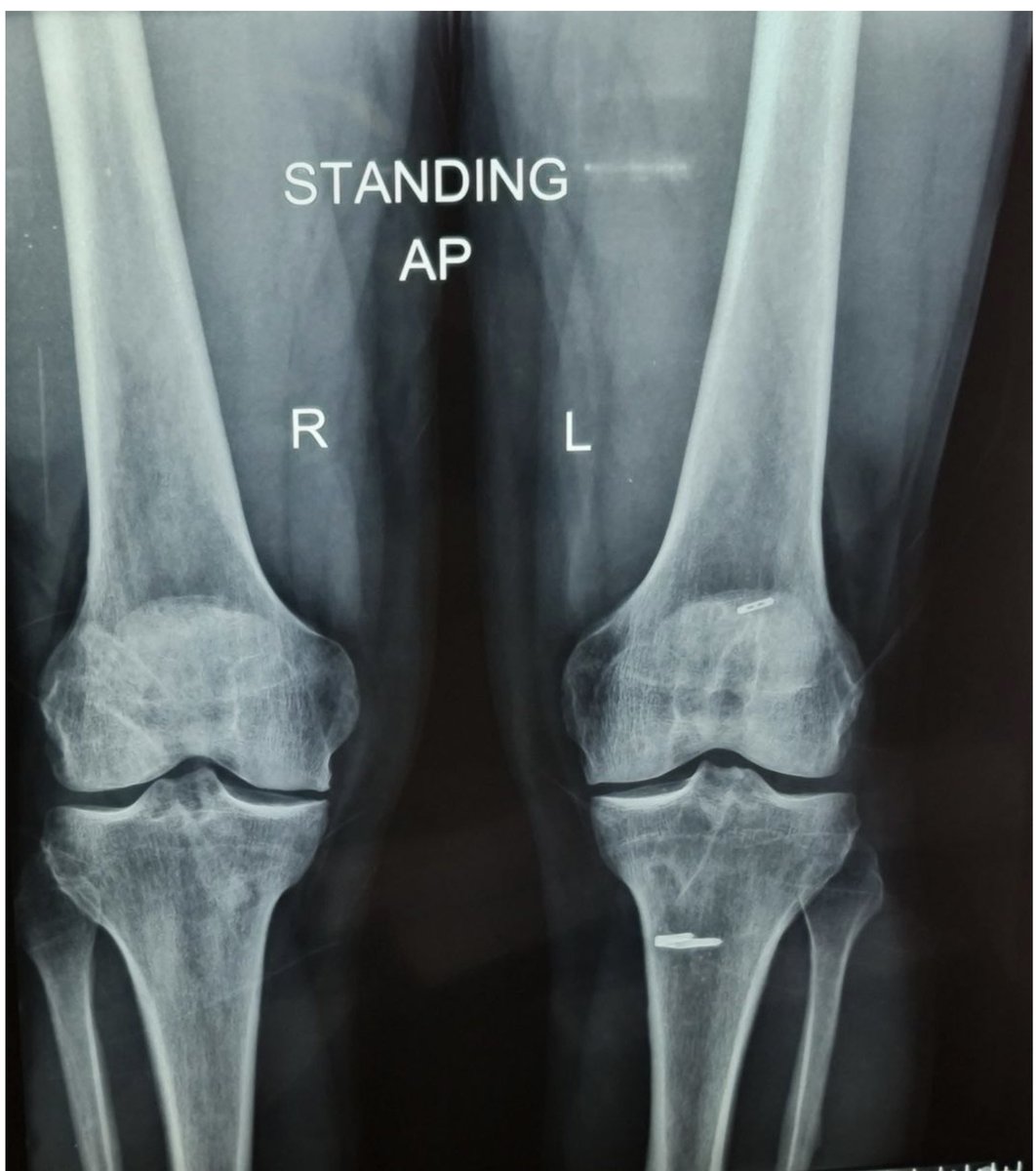
@DrNickColyvas for me ( anatomic guy ) i consider that as challenge to search more and it proofs that the right fact about ACL and its reconstruction is still unclear , I’ve the X-ray but I couldn’t upload it , thanks for sharing
English
@DrNickColyvas last case with interesting scenario i saw , the right knee was done with what we call anatomic technique , the left knee transtibial , the fun that he told me the left knee is doing great and his problem mainly in right knee, when i tested the stability it is more in left
English

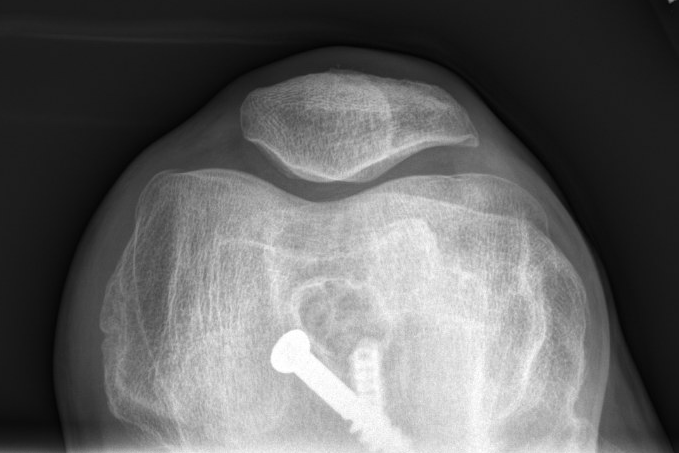
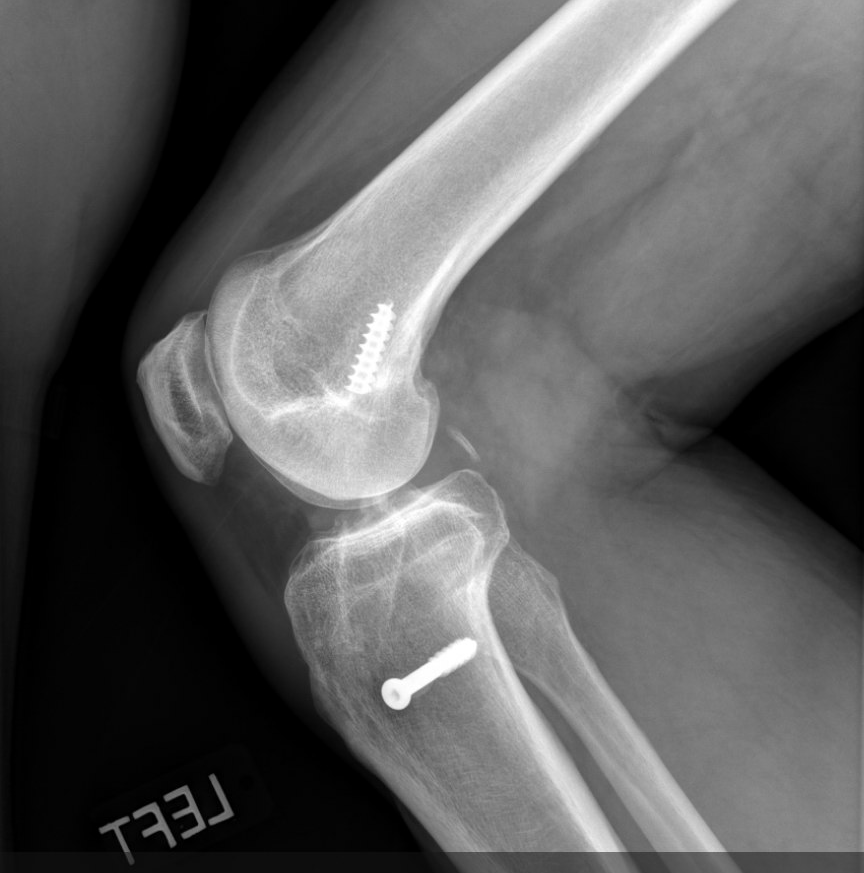
Another case of an ACL done with what we would consider unacceptable tunnel placement, who has been very active and happy on this knee for almost 25 yrs post surgery ...

English
@hjluks Thanks for sharing, regarding PGA/PLA what is your comment on using titanium screw on soft tissue graft tibial side only ,thanks in advance
English
Beware of the latest, greatest and “state of the art”…
Goretex ACL
Collagen meniscus implant
Metal on metal joints
Titanium joints
Double bundles
PGA/PLA screws
Shrinkage
Subacromial balloons
SCRs
Groove deepening procedures.
….
This list could go on and on…
English
@DrGadgil @hugortopedista @pratikorho @traumaticum Dear colleagues who voted for retro , haven’t you had any issues with knee pain after retro ?
Even after ante grade many patient develop knee pain and issues with motion in the first months
I am curious about retro when i open the knee !!
Thanks for sharing
English

What should be implant choice in this 26yr male with Distal 3rd femur shaft fracture.#MedTwitter @hugortopedista @pratikorho @traumaticum

English

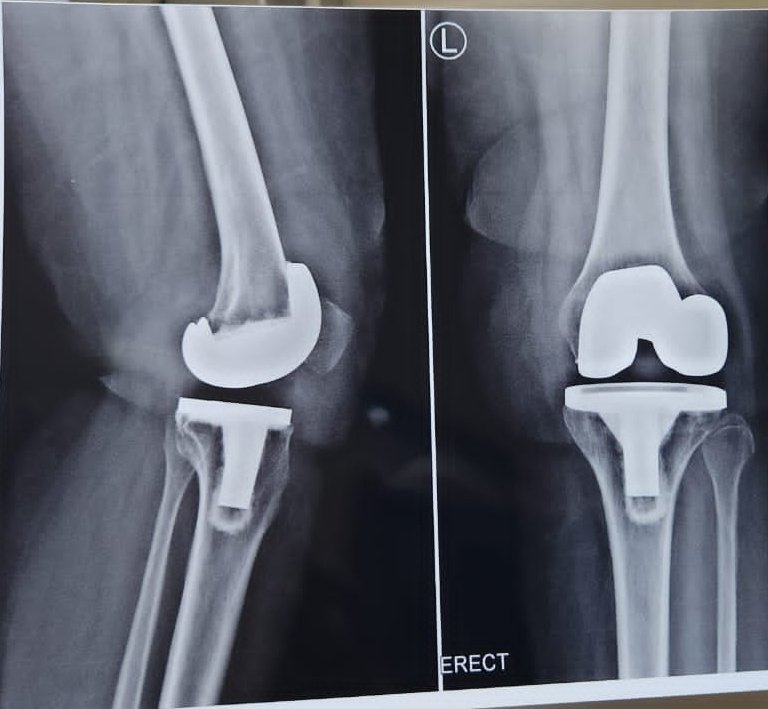
Hello #orthotwitter
55 y/o F, 3 mo post-op, pain with WB since 1 mo.
PMHx unremarkable, non-smoker. Pain constant, ↑ with ambulation, ↓ with rest, ↑ with flexion >90°
Neutrophils 72
ESR 45
CRP 10
PCT normal
Thoughts?
@kneedoclond @EdinburghKnee @aberizzi @drsebheaven
English
@NuelleSportsMD Absolutely I love this setup , and I would never use leg holder,
Better exposure
Easy drabs
On off tourniquet
Better for meniscus repair ( in out )
Libya 🇱🇾 English
ACL Friday!
ACL surgery set up that does not require a leg holder and does not require dropping the leg below the level of the bed. Also can be performed w/a single lateral side post.
English
@hjluks And for how long we can wait ? I mean is there a definite time to operate if not healed ?
English


ACL Friday!
The ACL can have a wide footprint on the femur. Where do you drill your femoral tunnel for a reconstruction?
1️⃣central
2️⃣towards AM bundle origin
3️⃣towards PL bundle origin

English
@darrenjohnsonmd @PittTweet Thanks doctor , could you thankfully draw for us where it should be on this image
Thanks in advance
English

AM to AM, study long ago from @PittTweet showed that is the best at controlling the pivot.
Clayton Nuelle, MD, FAAOS@NuelleSportsMD
ACL Friday! The ACL can have a wide footprint on the femur. Where do you drill your femoral tunnel for a reconstruction? 1️⃣central 2️⃣towards AM bundle origin 3️⃣towards PL bundle origin
English
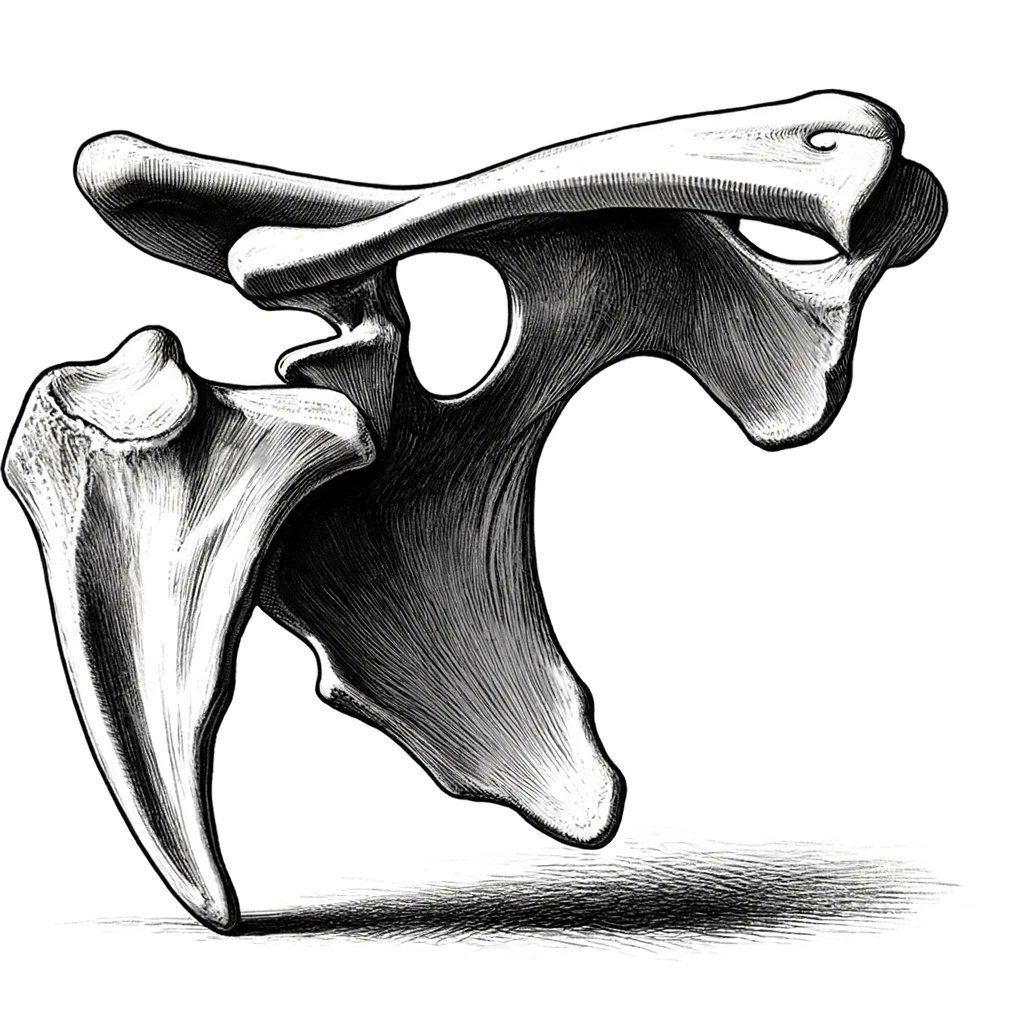
Orthopedic Truths: #6
Bone spurs in the shoulder
Disclaimer: I am firmly in the Save the Acromion club :-)
Many decades ago (1972), a famous shoulder surgeon proposed that an anterior spur on the acromion caused rotator cuff disease.
Somehow, that morphed into the cause of much shoulder pain for a short while.
Back in the day, we took the anterior portion of the acromion from many people, young and old alike.
Interestingly... the 1972 paper that spurred all the interest wasn't peer-reviewed.
But that didn't matter.
Hundreds of thousands of acromion have been harmed due to this paper 🤣
In this culture, the acromion has been metaphorically aggrieved.
The acromial shape changes over time.
However, most papers show that it doesn't have a role in the etiology of cuff tears.
Back in the days of open surgery, if you ran your finger in the subacromial space (SubAc) you found it to be smooth.
You didn't feel a spur.
That's because the spur lies within the CA ligament.
Hence, it dives medially as it heads distally.
Thus, away from the tuberosity and cuff enthesis.
We have traction spurs within ligaments all over our bodies.
We blame tendinosis, tendinopathy, overload, overuse, etc. for pain in many tendons throughout our body...
Yet we have blamed the acromion for all that ails the subacromial space for decades.
Just bizarre.
It never made sense.
The space between the tuberosity and the acromion increases beyond 60-80 degrees of elevation.
Yep, increases.
So pushing an arm up 160 degrees and claiming the pain is due to a spur doesn't sit well.
In full forward elevation, the acromial-humeral distance is at its widest.
Attempts by Christian Gerber and others have shown that when you build up the acromial undersurface to reproduce cuff tears, it always led to bursal-sided fraying and tears... as one would expect.
But that's not what happens in real life...
Where do most "tears" initiate?
Are they even "tears" if there's no trauma?
Anyway, I digress.
We know that most tears begin on the articular surface of the anterior SST.
So... if you're rubbing the upper surface, how would you tear the deep surface?
You don't
These cuff lesions occur for many reasons...
That's for another session.
There was a recent paper that showed that the recurrence rate of cuff tears was a little lower in the acromioplasty group.
But we can't assume it's due to a mechanical effect.
Many other papers...
Many, many, many other papers have shown that acromioplasty has a limited role in the etiology, progression, or recurrence rate of cuff tears.
Why is an acromioplasty still done?
idk
Do I do them?
Honestly, no.
If you do it for visualization, you should work on the scope position and portal placement.
You can't look at the subacromial space in an anesthetized patient and claim it's narrow!
Aside from cuff tear arthropathy patients... 😳
The distance of the SubAc space is dynamic.
It's not static.
Thus, if the cuff is paralyzed... well, you know.
Cuff weakness leads to narrowing dynamically.
If we want to improve the space, we should improve that.
If we whack the acromion---within a year...
If the cuff is still weak...
The head could simply elevate further into the defect.
We have all had patients with subacromial-based pain proven by injections, etc.
Yet they don't have tears.
Many improve with time, injections, and physio
But some don't.
It took a long time to adjust to not touching the acromion...
But these folks improve by just dealing with the bursa...
Or perhaps one day, we'll find out it was a placebo effect.
Over the last decade, a few sacred ortho procedures have not held up well against sham surgery studies.
But either way, these folks feel better despite keeping their acromion intact.
Besides, taking out the CA ligament could have serious implications.
If you've ever seen someone with anterior superior escape...
You will never forget the role of the CA lig.
I can't believe it's been 52 years, and we still argue about this :-)
Honestly... in writing these posts, it's unfortunate how little we have progressed in much of our understanding and practice.
Yes... we have progressed... Don't @ me.
Maybe my expectations were too high...
Safe to say... SubAc pain is more commonly an intrinsic problem than any extrinsic compression.
But wait!!
The lateral acromion overhang does have a role.
But we're not taking it out because of that role.
The acromial index seems to be important... we can counsel patients about the risk of recurrence and similarly quiet our exuberance about fixing certain tears.
But... we still should preserve this structure.
Given the increasing prevalence of rTSAs and the incidence of acromial fractures, we should preserve that bone stock as much as possible.
It's been 52 years, and we're still discussing whether the acromion has a role ;-).
I just love that.
English
@hjluks Great, brave post doctor , thanks for that , still one issue that used to see a lot which is , last 20 ACLR I did 16 of them has big bucket handle tears with ACL , is this an excuse to advice for ACLR from the injury immediately especially in young active athletes
English
Orthopedic Truths #4
The ACL:
The ACL is important for some people to remain active.
Others tolerate its loss very well.
ACL tears are too common in sports.
ACL tear prevention programs exist... they work, yet community/ school sports don't utilize them.
ACL tears are more common in athletes participating in the same sport year-round.
ACL surgery, despite years of research and practice, remains an imperfect solution to a complex problem.
Do all ACL tears require surgery?
No
But yours might.
Your child should probably have it.
It's the secondary injuries we worry about.
What about adults?
Many do fine without ACL surgery.
Some don't.
But it often pays to wait and see.
Everyone's knee feels unstable initially.
Very often, that stability improves with time and physical therapy.
Therefore, for adults, you might want to wait before booking that surgery date.
Why is the surgery an imperfect solution?
Because the native ACL isn't a straight, single-diameter structure, but our reconstruction is.
Secondary injuries can include meniscus tears and cartilage injuries.
Those will increase the risk of developing arthritis.
The history of reconstruction is wild... and somewhat circular.
Back in the 80's and 90's we argued about which graft worked well.
We still have those arguments.
Now, we added the quad tendon graft to the argument.
Would I take hamstrings from a sprinting athlete... no, not really.
Am I a quad enthusiast? Not yet.
When the MOON group announces their data, then I might.
But it took 20 years for that to come out for hamstrings vs BTB.
BTB remains the gold standard... and will for a while.
But we tried Goretex.
We tried other things, too.
Those didn't end well.
Oh. We have this scope thing. Let’s keep reconstruction via one tunnel. Evolution be damned.
The ACL has had the same femoral footprint (attachment) for millions of years. But heck.
Let’s put that tunnel here.
It worked for some... but many failed.
We tried to repair them, but they failed.
We developed tools to place the ACL where nature intended it.
But going too distal seemed to increase the risk of re-rupture, too.
Now we cheat a little back up the wall on the lateral condyle.
We tried reconstructing both bundles—certainly, that would work better. I tried them, too, but that didn't work.
Fixation... we need screws. The metal screw worked very well. It was predictable and easy to remove.
Oh.. I hate seeing screws on the x-ray. Let’s use these awesome bioscrews.
Wow…, I haven’t seen a cyst that big before 😩
Sadly... those screws dissolved the bone around the graft, too.
Then, we devised some wild, stupid ways to secure the graft that make revision surgery challenging.
Thankfully, most of those are gone now.
Along the way, we thought we would save our patient's tissue by using cadaveric tissue or allograft.
There were disease-spreading issues early on.
But that got better.
Oops... they fail very often in kids.
We don't use them in kids anymore.
We can use them in adults.
(But your own tissue is better.)
Hey... It's been 30 years, so let's repair them again.
That still didn't work.
Hey... let's put this little sponge in the repair.
Okay... That might work... the jury is still out on this.
"ACL tears never heal without surgery."
But it appears that they do!
Enter the cross-brace protocol.
It's annoying for the patient.
It doesn't pay the surgeon as well.
But it appears to work. For some.
The jury is still out. More research is needed.
But... ACL tears can heal.
Rehab. “I let my patients return to sports in 6 mos”. 🙄.
Just don't!
Don’t mess with the biology of healing.
Kids should wait 12-24 mos to return to sports.
I don't think that most parents understand the recurrent tear rate.
Most kids I see out there are not properly/fully rehabilitated after surgery.
It's hard when our lovely insurance companies approve 8 PT visits for an ACL patient.
Multinational/well-researched protocols exist for the rehab of an ACL athlete.
But they're not used often.
Ah... this messy little ligament has generated reams of "research" over the years. Much of it is nonsense, but some solid data exists.
The controversies around how to manage these athletes persist.
I would have thought we would have been further along, but here we are.
Stay tuned... I imagine we are still having the same conversations in 20 years.
Ask your school to implement ACL tear prevention programs.
English