Atherosclerosis retweetledi

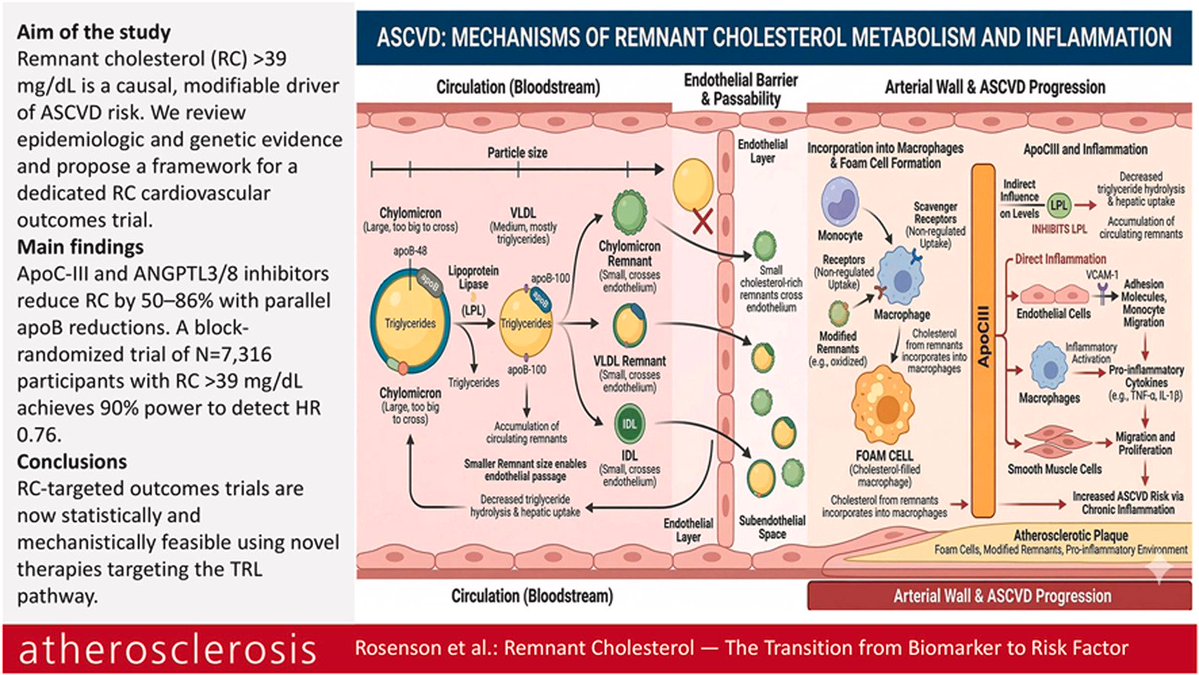
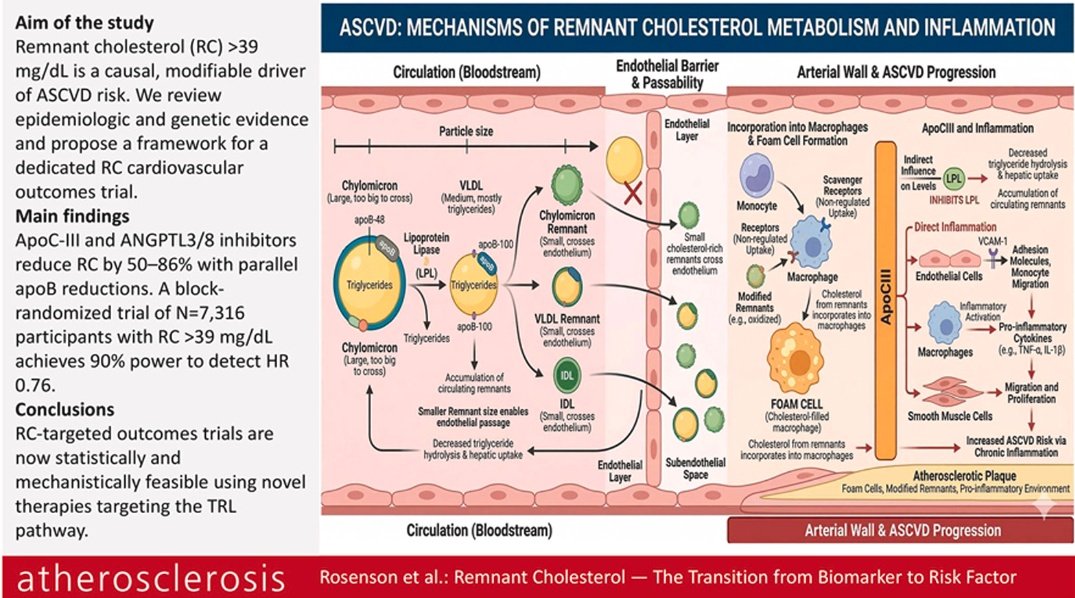
La epidemiologia, genética respaldan que TRL-RC es un factor causal y modificable del riesgo de evento
Debiéramos.priorizar agentes que reducen tanto la RC como la apoB e incluir a pacientes con niveles marcadamente elevados de TRL-RC
@EASCongress2026
atherosclerosis-journal.com/article/S0021-…
Español