Bryan Johnson@bryan_johnson
Your ankle is a window into your heart.
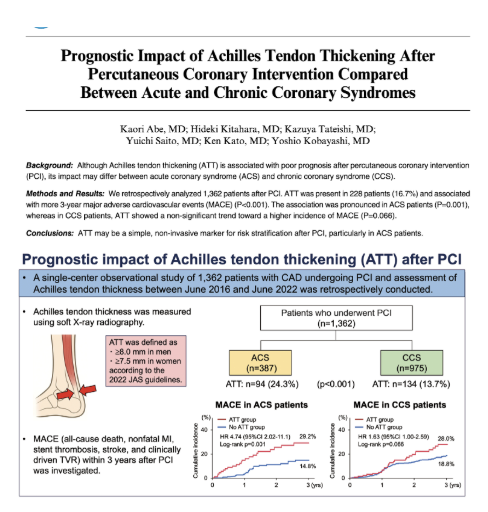
A new study found that patients with a thickened Achilles tendon were nearly twice as likely to experience a major cardiovascular event within three years of a coronary stent procedure.
An observational study retrospectively compared outcomes for 1362 participants with coronary artery disease undergoing PCI, examining differences between patients with and without Achilles tendon thickening (defined as ≥8 mm in men or ≥7.5 mm in women).
Patients with thickened Achilles tendons faced a 99% higher risk of major adverse cardiovascular events (MACE) over three years (28.4% vs 17.9% for those with and without thickening, respectively).
(MACE was defined as all-cause death, nonfatal myocardial infarction, stent thrombosis, stroke, and clinically driven target-vessel revascularization.)
Thickened Achilles tendons were more prevalent in patients with the more severe, rapidly developing, and less stable acute coronary syndrome (ACS) (24.3% had thickened tendons) compared to patients with the more stable chronic coronary syndrome (CCS) (13.7% had thickened tendons).
Among ACS patients, having a thickened Achilles tendon was a significant predictor, increasing the risk of a recurring major cardiovascular event within the next three years by 4.7 times.
The findings suggest that Achilles tendon thickening may serve as a prognostic marker in patients with cardiovascular disease, with special value in predicting early recurrence of major adverse cardiovascular events in patients with acute coronary syndrome.
While the analysis did not include blood cholesterol levels and does not establish causation, one plausible explanation is that Achilles tendon thickening reflects cumulative exposure to elevated LDL cholesterol over many years. This may be especially relevant in familial hypercholesterolemia, a genetic disorder characterized by markedly elevated LDL cholesterol, in which Achilles tendon thickening is also used as a diagnostic criterion.