
ANDROMEDA-SHOCK
2K posts
ANDROMEDA-SHOCK
@AndromedaShock
MD, U De Chile; PhD, U of Amsterdam. Intensivist following the principles of physiology and humanism! Septic Shock! And Winter/Wine Lover😍😍
Santiago, Chile Katılım Haziran 2021
571 Takip Edilen7.9K Takipçiler

Dear friends! A reminder that this Wednesday at 9 AM Chilean time (GMT-4) we have the first colloquium of the ANDROMEDA-SHOCK network “25 years of septic shock resuscitation trials” Dr Ricardo Castro PUC Chile (free w/o registration). us02web.zoom.us/launch/jc/8864…
English
ANDROMEDA-SHOCK retweetledi

🫀In cardiogenic shock, we still focus heavily on MACROcirculation:
📉 blood pressure
📉 cardiac output
📉 LVEF
📉 vasopressor dose
But what if the real battle is happening deeper?
🩸 At the microcirculatory level.
This excellent ATS viewpoint highlights one of the most important evolving concepts in shock physiology:
⚠️ normalization of macrocirculation does not necessarily mean restoration of tissue perfusion.
Despite advances in cardiogenic shock management, mortality remains >40%.
Even more striking, up to 45% of deaths occur in patients with normalized cardiac index.
That disconnect may be explained by persistent:
🩸 microvascular dysfunction
🩸 impaired capillary perfusion
🩸 endothelial dysfunction
🩸 tissue hypoxia despite “acceptable” hemodynamics
The review reinforces that: Microcirculation is not a passive bystander.
It may be a central driver of:
• organ dysfunction
• lactate persistence
• shock progression
• mortality
Particularly interesting is the emphasis on simple bedside tools.
We often think microcirculation requires advanced devices, yet:
📌 capillary refill time (CRT)
📌 mottling
📌 ΔPCO₂
📌 lactate trends
still carry strong prognostic value.
A CRT >3 seconds at ICU admission was associated with worse outcomes, and combining CRT with the CardShock score achieved an impressive AUC of 0.93 for outcome prediction.
The article also reviews modern technologies:
🔬 handheld vital microscopy
🔬 sublingual microcirculation imaging
🔬 NIRS
🔬 laser Doppler assessment
bringing “real time” bedside microcirculatory monitoring closer to clinical practice.
One of the strongest physiological messages:
⚠️ Shock is not only about flow. It is about effective tissue level oxygen delivery.
The review beautifully summarizes the four major mechanisms of microvascular dysfunction:
• heterogeneity
• hemodilution
• congestion
• edema
Particularly relevant for intensivists:
📌 venous congestion itself may worsen microvascular flow
📌 elevated filling pressures impair driving pressure
📌 edema increases oxygen diffusion distance
This is highly relevant in:
• advanced heart failure
• VA ECMO
• mixed shock states
• fluid overloaded patients
Another important takeaway: Persistent microcirculatory dysfunction after VA ECMO initiation was associated with increased mortality, even when macrocirculation improved.
Perhaps the key message of this paper is:
🩸 Microcirculation should no longer be considered a secondary endpoint in cardiogenic shock.
It may become one of the most important physiological targets of the next decade.
📖 Merdji H, American Journal of Respiratory and Critical Care Medicine. 2026, 212(3), 410–413 doi.org/10.1093/ajrccm….

English
ANDROMEDA-SHOCK retweetledi


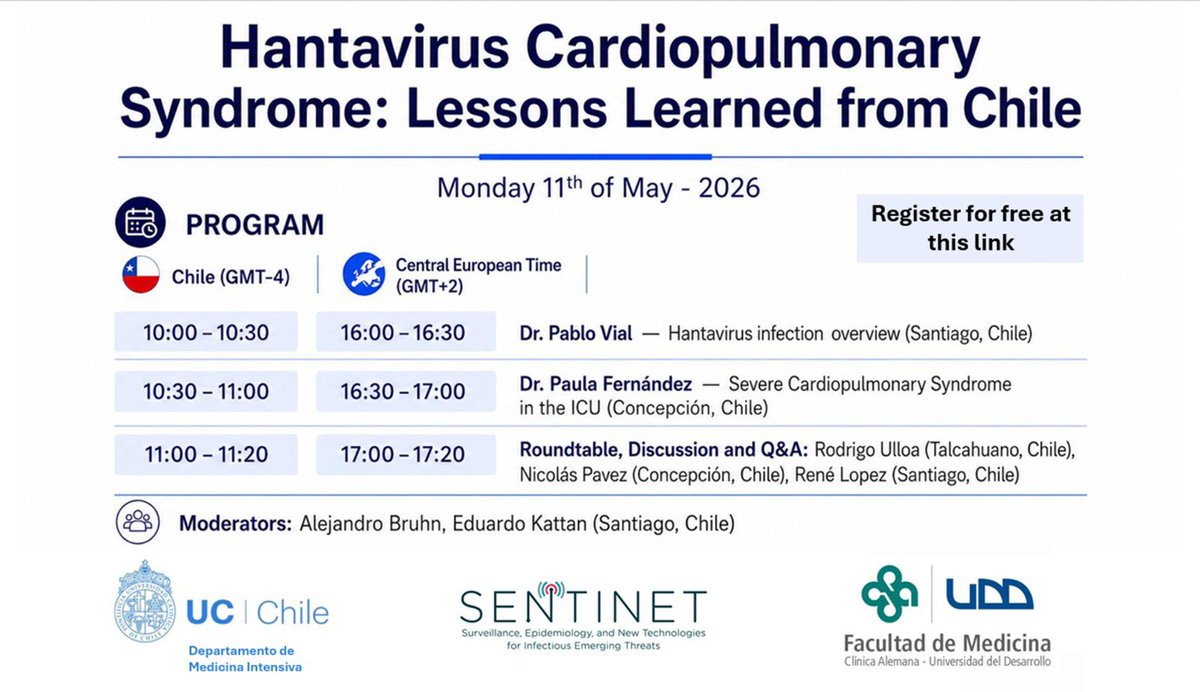
Webinar “Hantavirus Cardiopulmonary Syndrome: Lessons Learned from Chile”.
🗓️ Lunes 11 de Mayo 2026
⏰ 10:00 horas, (GMT-4)
Modalidad: Online, Gratuita.
Inscripciones: forms.gle/H6pJWVPm4j3MCd…
English
ANDROMEDA-SHOCK retweetledi

重症患者の気管挿管における循環動態の総説が、編集後のPDFとして見られるようになりました!
全文フリーでダウンロードできます👇
link.springer.com/article/10.118…

小谷祐樹 Yuki Kotani|集中治療医@YukiKotani5
重症患者の気管挿管における循環動態に関する総説が Journal of Intensive Care誌に掲載されました。 ・導入に伴う交感神経虚脱 ・挿管手技中の低酸素や無換気 ・陽圧換気への移行 などが循環生理にどう影響するかをまとめつつ、マネジメントの実際にも言及しました。 link.springer.com/article/10.118…
日本語

ANDROMEDA-SHOCK retweetledi

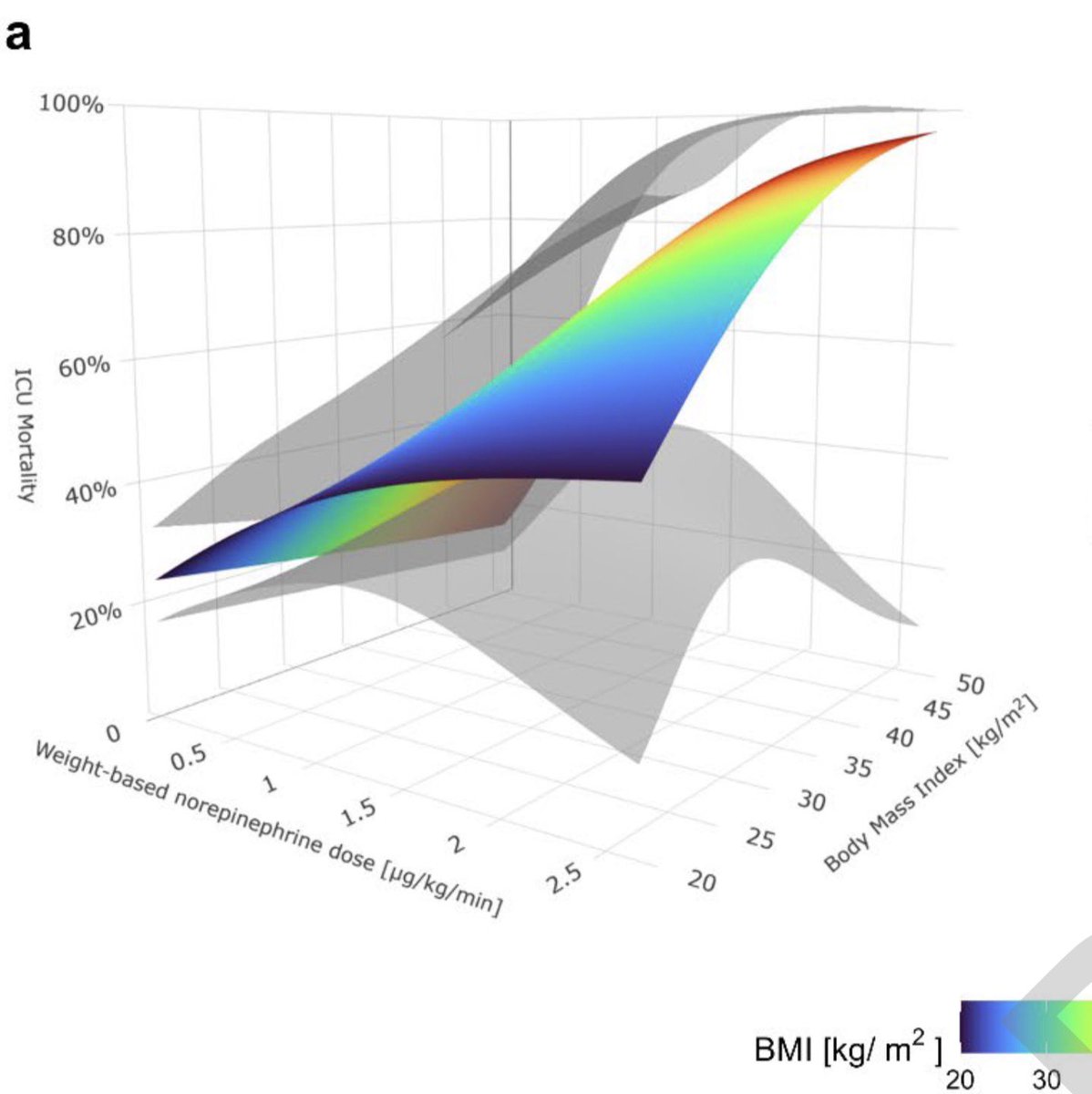
Do you titrate norepinephrine by weight-based dosing (mcg/kg/min) Well, you might be underestimating the predicted mortality by >20% in obese patients with septic shock. Absolute dosing (mcg/min) would be more accurate. Check our latest manuscript out in @_Anesthesiology
Eduardo Kattan@edu_kattan
@_Anesthesiology @DrMiguelIbarra1 @cjungMD @AndromedaShock @RCastro_L @smorales_a
English
ANDROMEDA-SHOCK retweetledi

Do you use norepinephrine with weight-based or absolute dosing strategies in septic shock pts? Does it really matter?
Check the results of our latest research published in @_Anesthesiology !
@DrMiguelIbarra1 @cjungMD @AndromedaShock @RCastro_L et al.!
journals.lww.com/anesthesiology…
English
ANDROMEDA-SHOCK retweetledi

El Estudio ANDROMEDA SHOCK-2 fue elegido como el Mejor Estudio Clínico de 2025 por el Editor de @JAMANetwork por su importancia (Choque Séptico, causa número 1 de muerte hospitalaria) e innovación (manejo por perfusión, resultado compuesto y jerárquico)
Si aún no lo has leído, qué esperas?
jamanetwork.com/journals/jama/…
Español
Just a first step on personalizing septic shock resuscitation! Without further emotional words thanks to all and also to JAMA for trusting and supporting us in the two ANDROMEDA trials so far!!
jamanetwork.com/channels/trials

English
Moments of pain and uncertainty trusting out good faith and motivation. On all the members of this amazing academic generated ANDROMEDA- Research Network with no funding but a tremendous heart! For this humble but strong positive signal after so many years of negative trials,
English
In this moment of emotion and joy, I can only think on the hundreds of wonderful investigators, residents, nurses that worked so hard on completing the trial guided by spirit, conviction, with the dream of improving care. On pts and relatives who accepted to participate in
English
During the next days will explain in a series of posts what AS2 is about: rationale, design, results, perspectives😍😍😍


English
ANDROMEDA-SHOCK-2 selected by JAMA as trial of the year 😍😍😍😍😍😍😍😍😍😍😍 jamanetwork.com/channels/trials
English
We are just submitting a Survey to >300 PIs and centers that participated in the ANDROMEDA-SHOCK Network studies!! The idea is to built up a comprehensive and dynamic database that helps our affiliates to plan future studies!! The Network is getting stronger and more to come!!
English
We are analyzing the results of ANDROMEDA-PEGASUS with 3150 recruited pts in 4 continents. We hope it provides a strong epidemiological support for considering pulse pressure to take initial decisions during septic shock resuscitation. Coming soon by the ANDROMEDA Network
English
Just out of the oven! Acute hemodynamic tests to determine the status of macro-to-microcirculatory coupling in septic shock. More and more validating data. In ANDROMEDA-SHOCK-2 great success in normalizing CRT with various tests (summarized in the text)! The way to personalize!!


English
ANDROMEDA-SHOCK retweetledi

Refractory septic shock is persistent hypoperfusion in a fluid-unresponsive patient requiring high-dose vasopressors (> 0.5 gamma/kg/min basal norepi equivalent) after appropriate resuscitation and after excluding other causes of shock.
Dr. Chacón-Lozsán F .'.@franciscojlk
🤔When does septic shock become “refractory”? We have used the term for years. But until now, we never truly agreed on what it means. A new joint Delphi consensus from SCCM and ESICM finally brings structure to one of the most critical, and most ambiguous concepts in intensive care And the message is powerful: Refractory septic shock is not defined by blood pressure. It is defined by failed physiology. Three key takeaways stand out. ->First, tissue perfusion is at the center of the definition. Not MAP. Not urine output. But persistent hypoperfusion: Elevated lactate Prolonged capillary refill time Even after adequate resuscitation. This is a major conceptual shift: we are moving from pressure-based resuscitation → perfusion-based resuscitation. ->Second, dose matters more than the number of drugs. The consensus highlights a threshold: norepinephrine equivalents > 0.5 µg/kg/min Not how many vasopressors you use, but how much support is required to maintain circulation. This reframes severity in a much more physiologically meaningful way. ->Third, and perhaps most important: Refractory shock requires proof that you did everything right first. Before labeling a patient as refractory, you must demonstrate: 1.Adequate fluid resuscitation 2.Lack of fluid responsiveness 3.Exclusion of other shock types using critical care ultrasound ->Only then, failure becomes “refractory.” There is also what the consensus rejects, and this is equally important: No fixed lactate cutoff No ScvO₂ No urine output No strict MAP threshold Because reality is more complex than a number. 🤓Final definition: Refractory septic shock is persistent hypoperfusion in a fluid-unresponsive patient requiring high-dose vasopressors after appropriate resuscitation and after excluding other causes of shock. Why this matters? This is not just semantics. A clear definition means: Better patient stratification More meaningful clinical trials Earlier recognition of the sickest patients And ultimately, more targeted therapies Because not all septic shock is the same. And the sickest patients deserve a name, and a strategy. 📃Reference Leone M Intensive Care Medicine. 2026. doi.org/10.1007/s00134…
Assago, Lombardia 🇮🇹 English