Lee Berry retweetledi
B-lines are most often discussed in the context of pulmonary edema. But the spacing between them carries a different kind of information — one that reflects structural lung disease rather than fluid overload.
English
Lee Berry
3.2K posts

@Bezza_lee
RN , ACCP, USS and POCUS enthusiast. Deluded football player / manager. Ex 90s dance child.



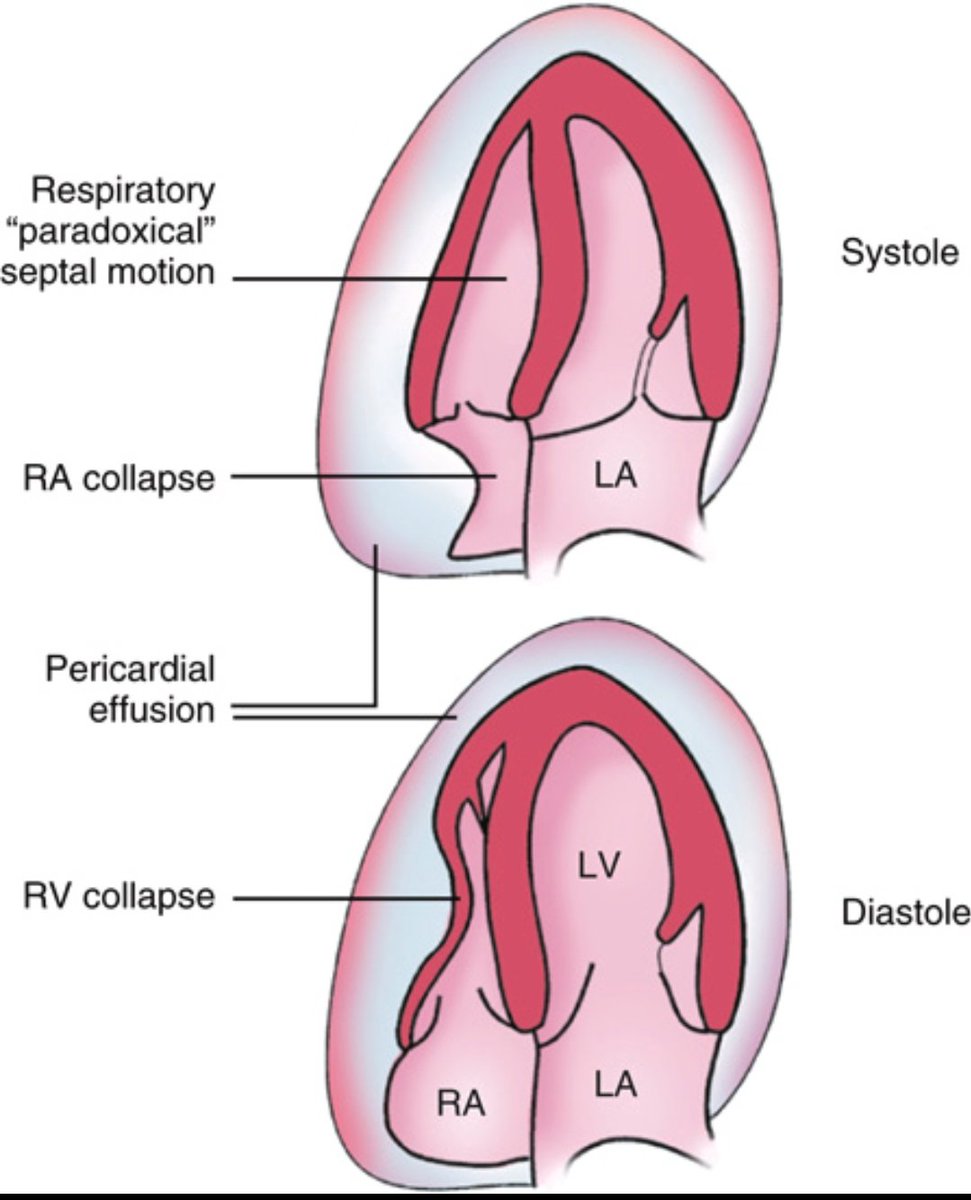
The heart is struggling to fill and pump blood. What’s your diagnosis?