Camila Peña retweetledi

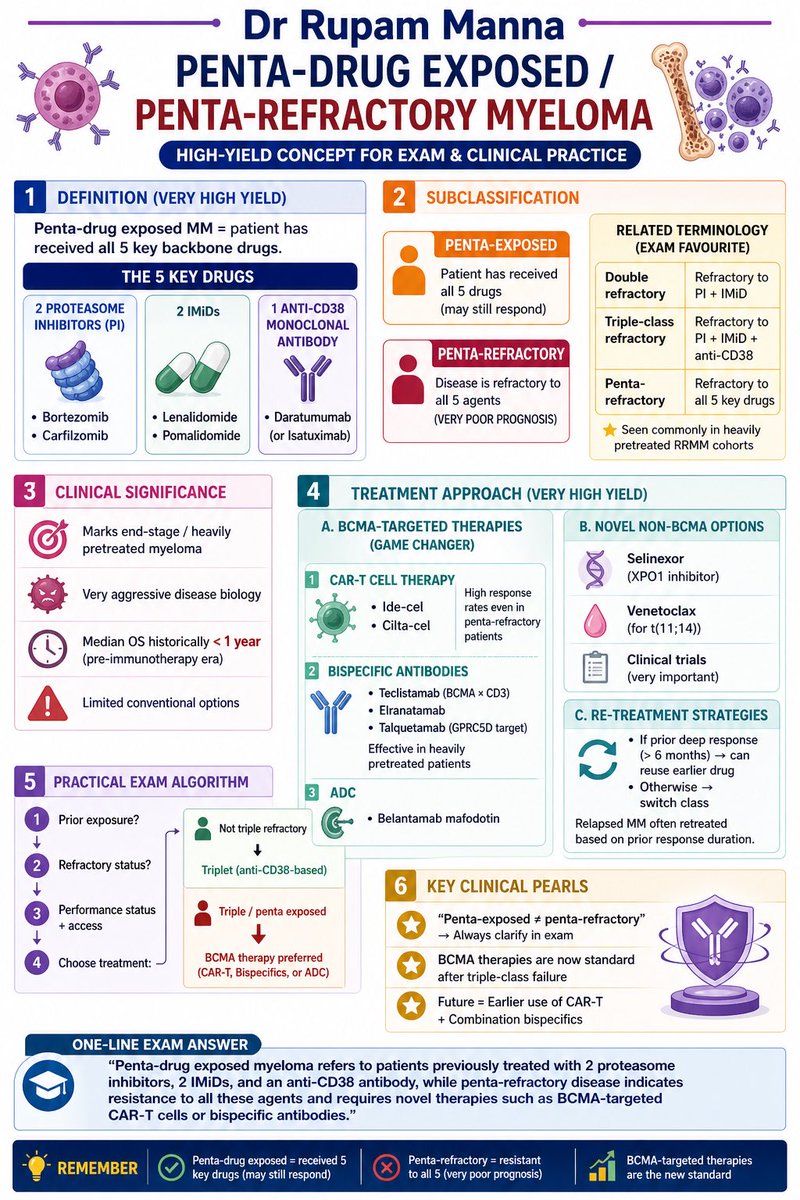
PENTA-DRUG EXPOSED vs PENTA-REFRACTORY MYELOMA — MUST KNOW 🔥
End-stage myeloma is no longer the end.
💡 Know the difference
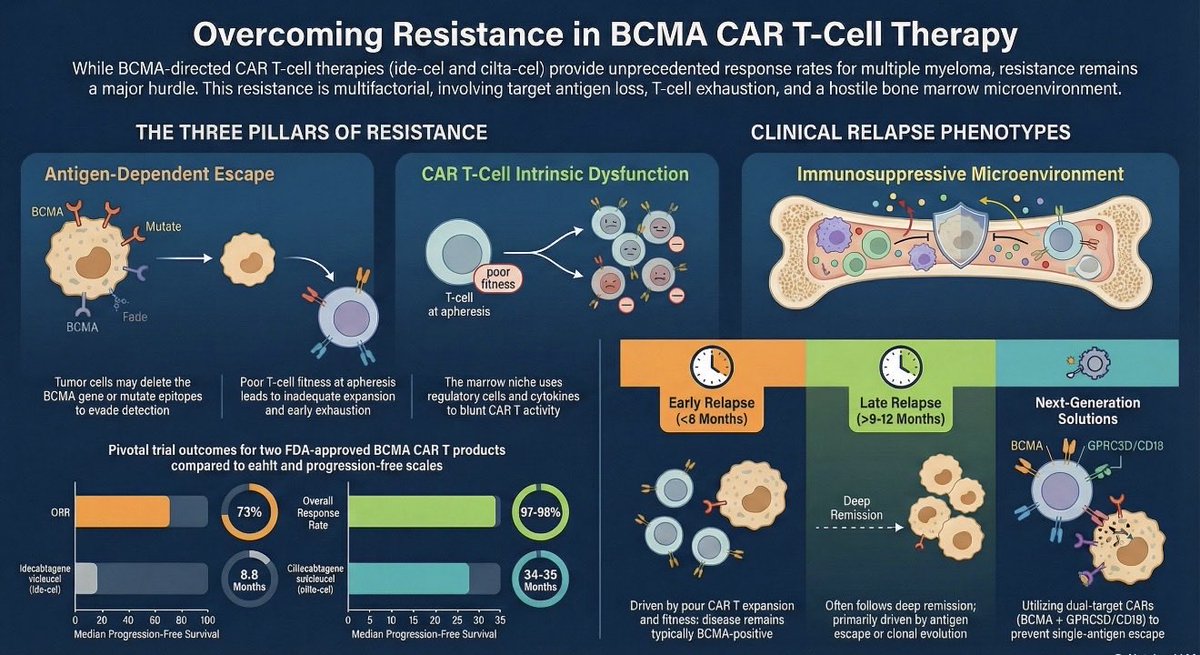
💡 Understand resistance patterns
💡 Use BCMA-targeted therapies smartly
From CAR-T to bispecifics — this is where modern oncology is changing survival 🚀
👉 Exam + clinic ready in 1 slide
#MultipleMyeloma #Hematology #Oncology #MedEd #FOAMed #MedicalEducation #CancerCare #CAR_T #BispecificAntibodies #BCMA #RRMM #DrNB #DMOncology #MedTwitter #OncoTwitter
English