
CommsC4TS retweetledi

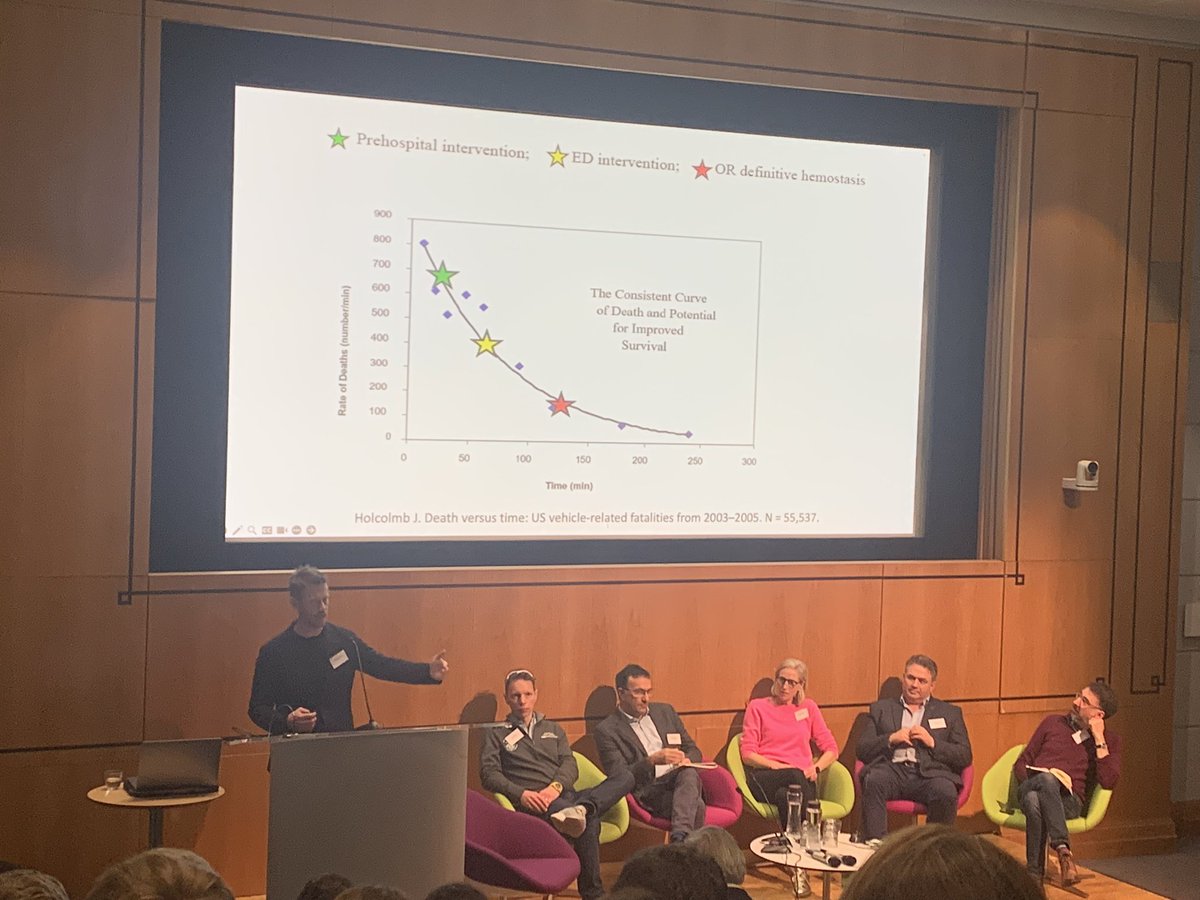
We’re looking forward to working with our colleagues @QMUL @aberdeenuni @NHSBartsHealth @LDNairamb @Ldn_Ambulance @KingsCollegeNHS @geshNHS @ImperialNHS to assess how the system can support doctors helping seriously injured Londoners.
English