Daniel Peters retweetledi

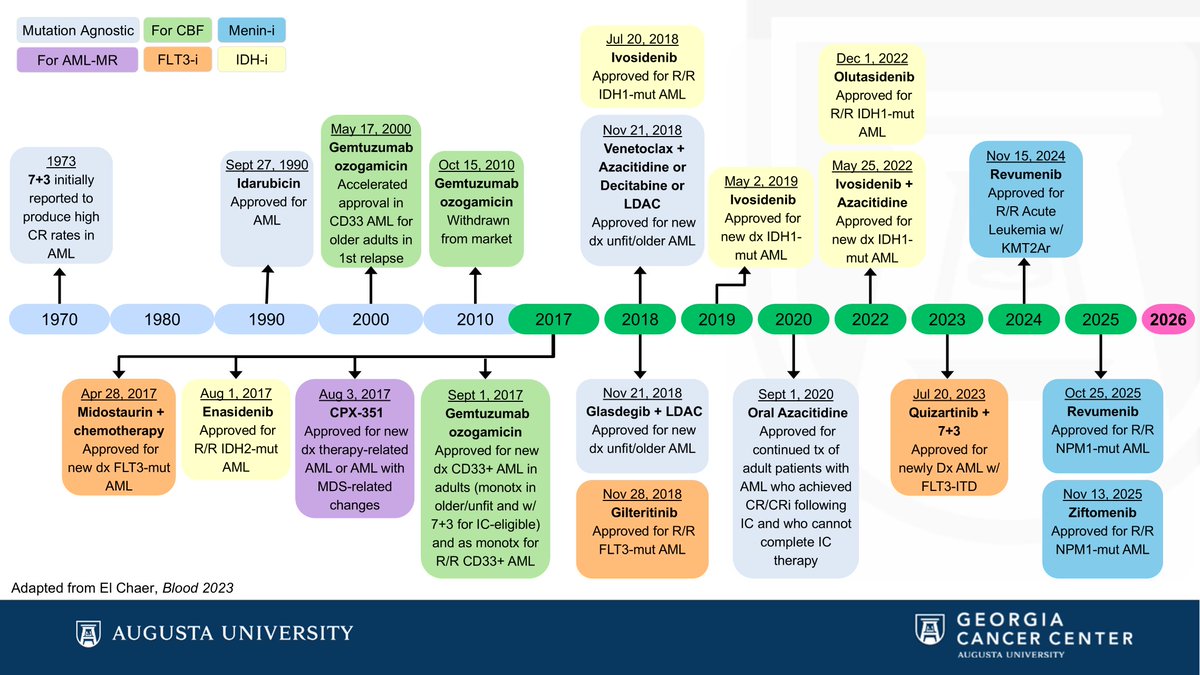
Azacytidine, our fantastic hypomethylating agent, used for treatment of MDS and AML, was discovered in 1964, and then fell into oblivion. Almost 40 years later it was FDA approved as the first effective MDS treatment.
A 🧵about an unusual revival:
English