Sabitlenmiş Tweet
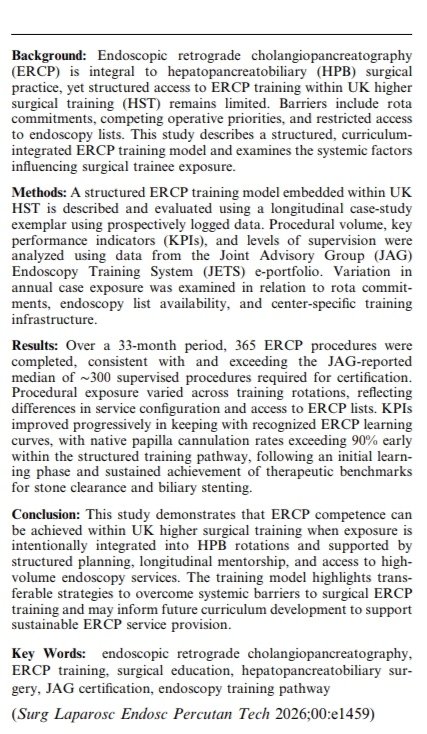
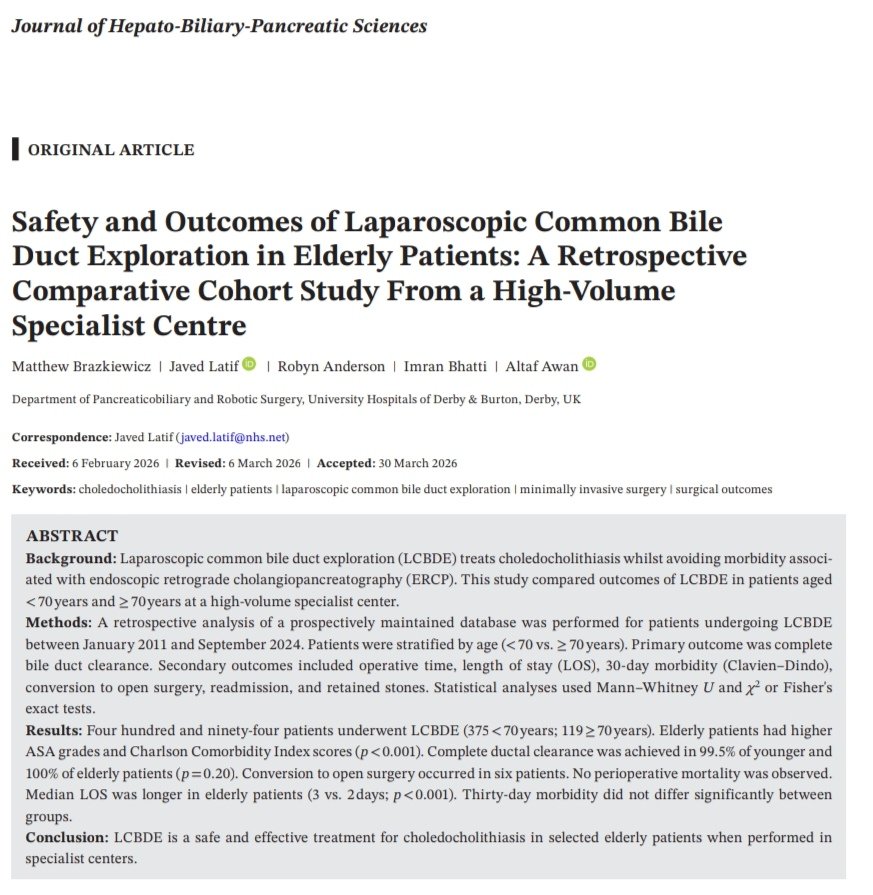
Pleased to share our latest publication in @JSHBPS Journal of HBP Sciences on the Safety and Outcomes of LCBDE in Elderly Patients.
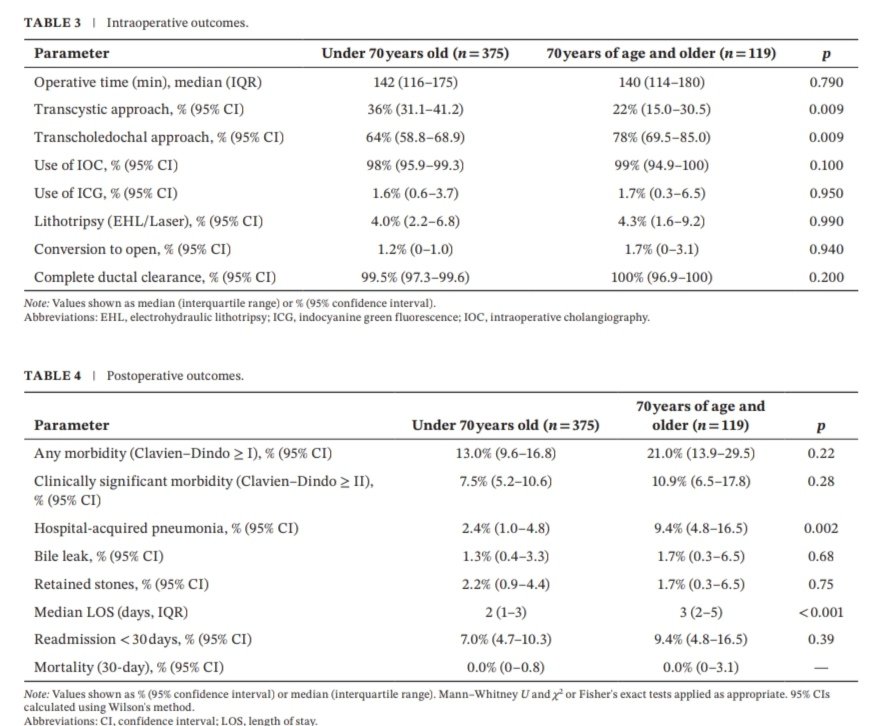
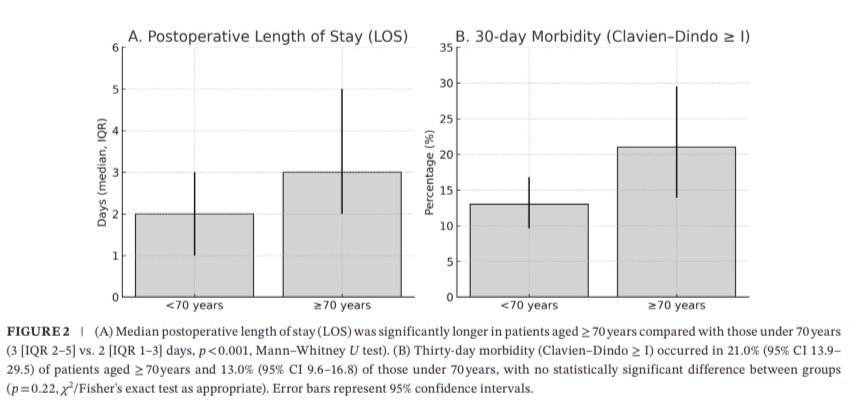
In 494 patients, outcomes in ≥70 vs <70 years were equivalent despite higher comorbidity, with ~100% duct clearance, no mortality, and similar morbidity. LOS was slightly longer in the elderly group.
LCBDE remains a safe, definitive single-stage approach and age alone should not preclude LCBDE in specialist centres.
Link to paper:
onlinelibrary.wiley.com/share/author/J…

English