Sabitlenmiş Tweet
Future
1.8K posts


Future
@Doc_Hieu
Critical Thinker, Explorer. 🇮🇸 🇪🇨 🇨🇷 🏴 🇫🇷 🇮🇹 🇳🇱 🇩🇰 🇳🇴 🇸🇪 🇨🇦 🇯🇵 🇻🇳 🇹🇭 🇩🇪 🇮🇪 🇲🇾 🏴 🇧🇪 🇬🇷
United States of America Katılım Şubat 2015
142 Takip Edilen787 Takipçiler

Future retweetledi

#dcvax $nwbo #gbm
Some interesting synergy with these industry updates of companies in the session that George Zavoico, PhD, $nwbo chairs with analysis below along with details of day 2 Opening keynote address by Ira Mellman PhD, Parker Institute for Cancer Immunotherapy
Agenda
Frontiers in Cancer Immunotherapy
Monday, 22 June 2026, 08:30 - Tuesday, 23 June 2026, 17:20
Session II: Brief Industry Updates
Chairperson: George Zavoico, PhD, Northwest Biotherapeutics
12:45
Metabolic mechanisms of resistance to cancer vaccination
Lisa Butterfield, PhD, Consultant
1:05 PM
Leveraging Synthetic Antigens to Create Universal Immunotherapies for Solid Tumors
Lex Johnson, PhD, Dispatch Bio
1:25 PM
Robert Fenstermaker, MD, MimiVax
1:45 PM
Introducing Normunity’s Immuno-Smart Targets: Novel Immuno-Relevant Tumor-Specific Targets to Optimize the Safety and Efficacy of Payload-Carrying Biologics
Rachel Humphrey, MD, Normunity
The presentations scheduled for this session offer several points of technical synergy with the DCVax (L-Dendritic Cell) platform technology, particularly regarding the enhancement of its efficacy within the immunosuppressive tumor microenvironment.
Synergies with DCVax Platform Technology
1. Overcoming Metabolic Resistance (Dr. Lisa Butterfield)A primary challenge for dendritic cell vaccines like DCVax-L is the metabolic hostility of the tumor microenvironment (TME). Tumors often deplete essential nutrients (like glucose and amino acids) and produce immunosuppressive metabolites (such as lactic acid), which can impair the maturation and function of the injected dendritic cells.
Synergy: Understanding these metabolic "brakes" could lead to combination protocols where DCVax-L is administered alongside metabolic inhibitors. This would ensure that the dendritic cells can effectively prime T-cells without being silenced by the tumor's metabolic defenses.
2. Universal Immunotherapies and Synthetic Antigens (Dr. Lex Johnson)DCVax-L is inherently personalized, utilizing the full spectrum of a patient’s own tumor lysate (proteome).
Synergy: Research into synthetic antigens could complement the DCVax approach by providing "booster" targets. If universal antigens can be identified that are common across solid tumors, they could potentially be loaded onto the DCVax platform alongside the patient-specific lysate to ensure a more robust and sustained immune response.
3. Targeting the "Immuno-Smart" Proteome (Dr. Rachel Humphrey)Normunity’s focus on tumor-specific targets for payload-carrying biologics (like ADCs) aligns with the need for precision.
Synergy: If "Immuno-Smart" targets can identify specific vulnerabilities in the tumor's exterior, these could be used as markers to track the success of DCVax-induced T-cell infiltration. Furthermore, using biologics to "de-bulk" or weaken the tumor's structural integrity could make it more susceptible to the systemic immune surge triggered by a dendritic cell vaccine.
Strategic Context: Dr. George Zavoico and NWBO
The presence of Dr. George Zavoico as the Chairperson for this specific session is significant for Northwest Biotherapeutics ($NWBO) for several reasons:
Scientific Leadership: As a PhD and a key figure at Northwest Biotherapeutics, Zavoico’s role in moderating these specific topics—resistance mechanisms, synthetic antigens, and novel targets—places $NWBO at the center of the conversation regarding the next generation of immunotherapy.
Integrated Approaches: His oversight of these "Brief Industry Updates" suggests a strategic interest in how DCVax might integrate with these emerging technologies. For example, if DCVax-L provides the "engine" for the immune response, the technologies presented by Normunity or Dispatch Bio might provide the "navigation" or "fuel" to overcome localized resistance.
Validation: Serving as a chairperson at a New York Academy of Sciences (NYAS) event reinforces the company’s standing within the academic and regulatory community, particularly as they navigate the transition from clinical trials to potential market integration and synergistic trial designs.
Day 2 - Opening Keynote Address
9:05 AM
The coming renaissance of cancer immunotherapy
Ira Mellman, PhD, Parker Institute for Cancer Immunotherapy
events.nyas.org/cancerio26/age…

English
Just to be clear, I could care less what the #NWBO daily up and down is, what I care about is the final price big pharma wants for my shares. Glad I accumulated while it was around 0.20 and would be happy for shorts and MM to push it down once more. MMs lazy POS, get it down!
English
Then ask AI to give you an estimate per share for buyout post MHRA approval with a turnkey manufacturing with Flaskworks and the Kalinsky IP and the patent for dendritic cells with PD1. Let me know what you find, #NWBO - I will wait. Post comments below.
Future@Doc_Hieu
Take a deep dive with AI on the Kalinsky IP and his work on turning cold tumors hot with Keytruda and why that is something BP want so badly given the 2028 patent cliff. #NWBO
English
Did canaccord give just money or gave up less money and promises to cooperate and snitch on the other MMs? #NWBO
Hoffmann@hoffmann6383
➡️A Settlement $NWBO The Case: Northwest Biotherapeutics, Inc v. Canaccord Genuity LLC, 1:22-cv-10185, (S.D.N.Y.) The Docket: courtlistener.com/docket/6657959… Recall, when I stated Canaccord Genuity was selling their market making division to Cantor and that could lead to a settlement as they would want to clean up before selling? See: x.com/hoffmann6383/s… Well, it happened. Just like TD settled their spoofing lawsuit prior to their Schwab sale. Here is $NWBO's recent court filing showing they have reached a settlement with Canaccord Genuity: See attached image. This should give $NWBO an infusion of cash. As a public company we should keep an eye on upcoming 10Q/10K filings to get an idea of the settlement amount.
English
If there was a canaacord #NWBO settlement - wouldn’t NWBO not want to divulge as it may set a precedent and limit payout by other parties in regards to figuring out damages? Thoughts @hoffmann6383 ?
Kelly@Kelly712717541
NorthWest Biotherapeutics Inc : The Judge issued an order dated 4/30 sta... investorshub.advfn.com/boards/read_ms… via @Investors_Hub$nwbo. Not an attorney. Does this sound accurate?
English
@hoffmann6383 @StonkMasterJ How do you know for sure it’s a monetary settlement?
English


Oh @hoffmann6383 where art thou?
SemperFITrader@SouthernDrive21
@hoffmann6383 $nwbo NWBO Just Dimissed the case against one of the defendents "Canaccord Genuity LLC" "NWBO has agreed to dismiss with prejudice all claims asserted against Canaccord in the above-captioned action, without costs to any party" That leaves CITADEL SECURITIES LLC, G1 EXECUTION SERVICES LLC, GTS SECURITIES LLC, INSTINET LLC, LIME TRADING CORP., and VIRTU AMERICAS LLC
English
#NWBO commentary on demand for their product. Confidence in regulatory approval. Control of manufacturing processes.
Patricia Elvir Pons MD@ElvirPons
English
Future retweetledi





#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
English
Future retweetledi

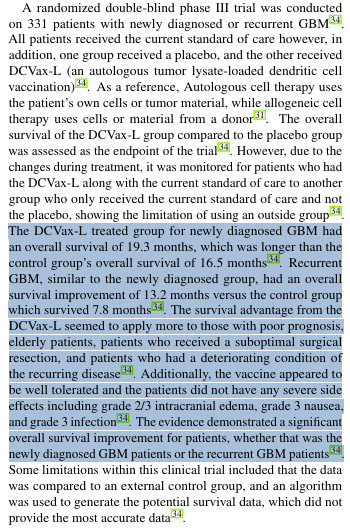
#DCVax-L: The evidence demonstrated a significant overall survival improvement for patients, whether that was the newly diagnosed #GBM patients or the recurrent GBM patients
💪
BeProactive
FreezeYourTumor
GetDCVax
QualityOfLifeMatters
#glioblastoma $nwbo
nhsjs.com/wp-content/upl…
English


$NWBO
Inexplicable delay?
No. We’re 103 days after CHM meeting two, the most complex cancer treatment in assessment, thus still in approval window.
GIF
English
@andrewcaravello @metacollectiveG He will be remembered for being part of the good fight
English

Heartfelt condolences to the family and friends of Dr. Greg Zivic, a true friend and fearless advocate for truth. He helped spread the word about $NWBO and all it stood for with conviction and integrity. He will be greatly missed. Rest in peace, Dr. Zivic @metacollectiveG 😞😞😞
English
@andrewcaravello Yes, or that. It certainly validates what NWBO has been doing for years.
English
Dr. Robert Aiken’s public criticism of $NWBO #DCVax-L should be read with the relevant context disclosed up front, because his professional relationships overlap with multiple competing positions in the glioma treatment landscape.
Public Open Payments reporting shows industry payments to Dr. Aiken in 2024 from Novocure, the maker of Optune and Tumor Treating Fields, a product that competes for the same add on role in newly diagnosed glioblastoma. He also received payments from Servier Pharmaceuticals, a company expanding its footprint in glioma through targeted therapy development and commercialization.
Most directly, Dr. Aiken is a co investigator on a Phase 2 clinical trial evaluating DOC1021, an autologous dendritic cell vaccine developed by Diakonos Oncology for newly diagnosed glioblastoma at Atlantic Health. That program is not adjacent. It is a direct scientific and commercial competitor to the DCVax L platform. In public remarks about Diakonos, he has described the approach as momentous and as evidence of substantial momentum behind the science.
Against that backdrop, Dr. Aiken has framed DCVax L as a first generation dendritic cell vaccine. There is one narrow sense in which that label is accurate, and it actually strengthens the case for DCVax L rather than diminishing it. DCVax L was studied in a deliberately clean configuration. It was not paired with checkpoint inhibitors and it was not boosted with innate agonists such as TLR3 class adjuvants. That means the Phase 3 program functioned as a proof of concept for what an autologous, whole tumor lysate loaded dendritic cell vaccine can do as a standalone immune instruction platform, with fewer confounders and less attribution ambiguity than modern combination stacks.
At the same time, calling it a dead end is not a neutral scientific conclusion. DCVax L has completed a 331 patient Phase 3 trial with results published in JAMA Oncology, and the program has advanced into active regulatory review in the United Kingdom through an MHRA marketing authorization application. That is not the profile of a failed concept. It is the profile of the most advanced autologous dendritic cell vaccine in glioblastoma moving through a formal approval pathway.
Bottom line. Dr. Aiken’s financial relationships and his active role running a competing dendritic cell vaccine trial are not peripheral details. They are directly relevant context for interpreting his public posture toward DCVax L, especially when his commentary leans on generational branding while he is simultaneously championing a rival platform that has not yet produced Phase 3 outcomes.
openpaymentsdata.cms.gov/physician/3559…
Andrew Caravello, DO@andrewcaravello
He’s only correct in the sense that DCVax-L did not use any booster agents. That’s it. It was a phase 3 trial, and they were testing the vaccine by itself. They couldn’t add these booster agents later, that’s why all these newer trials show great evidence that it works fantastic. Over 60% survival.
English