Jean Bustamante-Alvarez MD MS retweetledi
Jean Bustamante-Alvarez MD MS
2.4K posts

Jean Bustamante-Alvarez MD MS
@DoctorJeangoB
Bronx, NY Katılım Şubat 2017
1.1K Takip Edilen620 Takipçiler
Jean Bustamante-Alvarez MD MS retweetledi

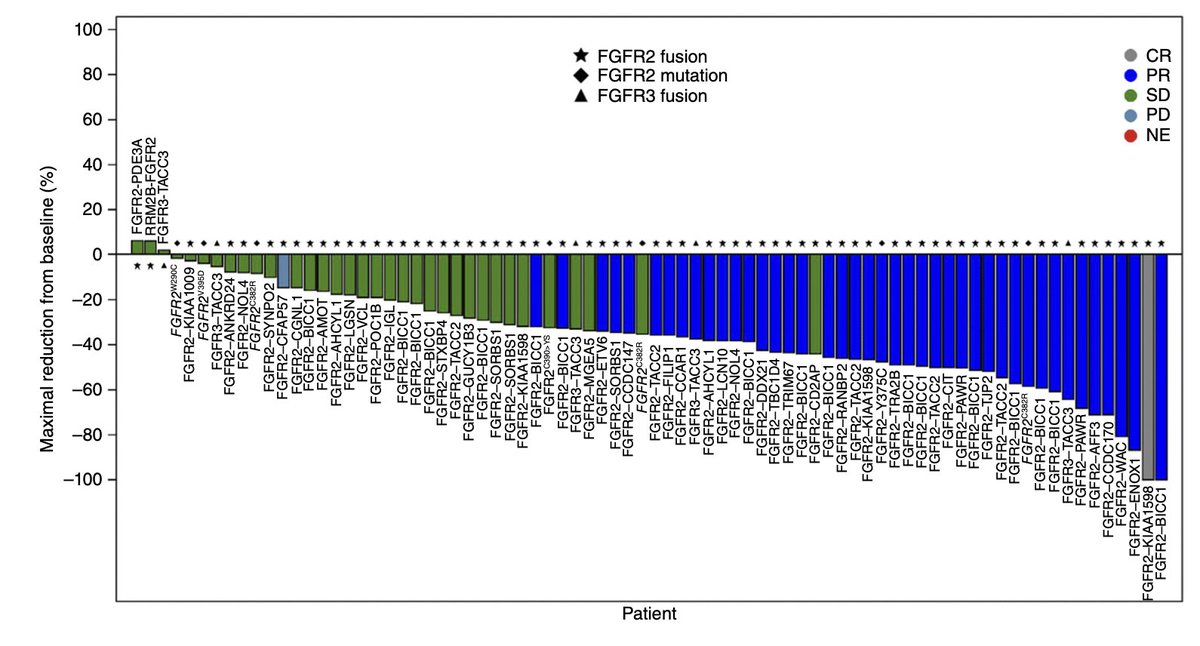
Clinical guideline for the diagnosis and treatment of fibrolamellar carcinoma
@HEP_Journal
doi.org/10.1097/HEP.00…
👏Timely guideline
👉still very difficult to treat tumor
@ASCO @myESMO @EASLnews @ILCAnews
English
Jean Bustamante-Alvarez MD MS retweetledi

Are B7H3 ADCs next for lung cancer?
Ph Ia/b trial of GSK5764227 @Cancer_Cell
- 237pts
- g3+ TRAEs ⬇️WCC, ANC, Hb
- ORR 52.3% ES-SCLC; 22.4% NSCLC
Pleased to be participating in Ph3 EMBOLD trial @CancerCentreIre 🇮🇪
@OncoAlert @cancertrials_ie #LCSM
cell.com/cancer-cell/fu…
English
Jean Bustamante-Alvarez MD MS retweetledi
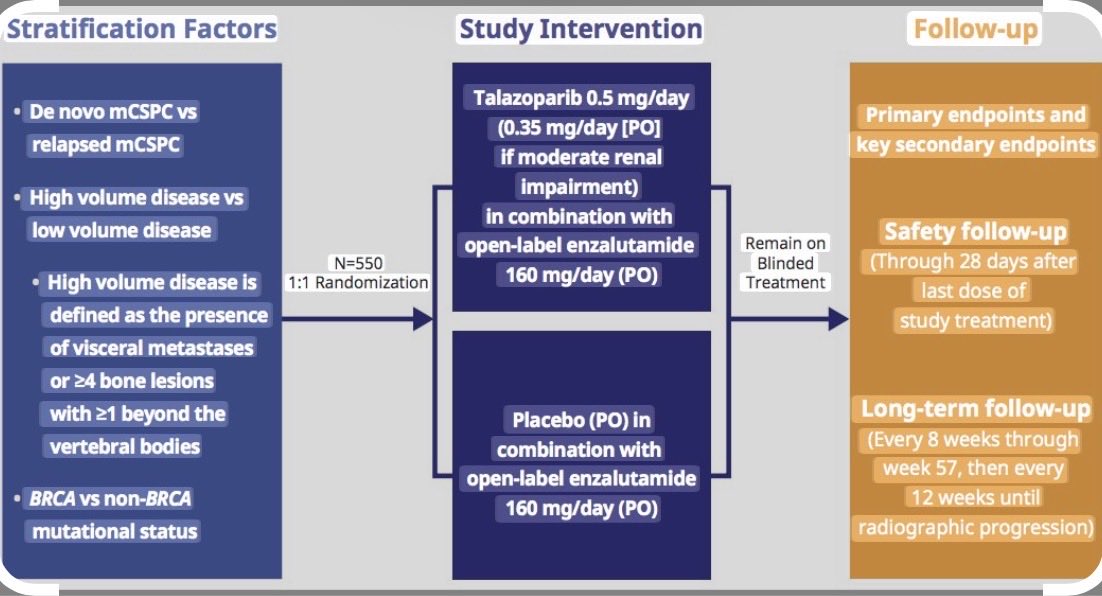
Just in: The phase 3 Talapro-3 trial met its primary endpoint!!!
fiercepharma.com/pharma/pfizer-…
@OncoAlert @AUC3_Official
English
Jean Bustamante-Alvarez MD MS retweetledi
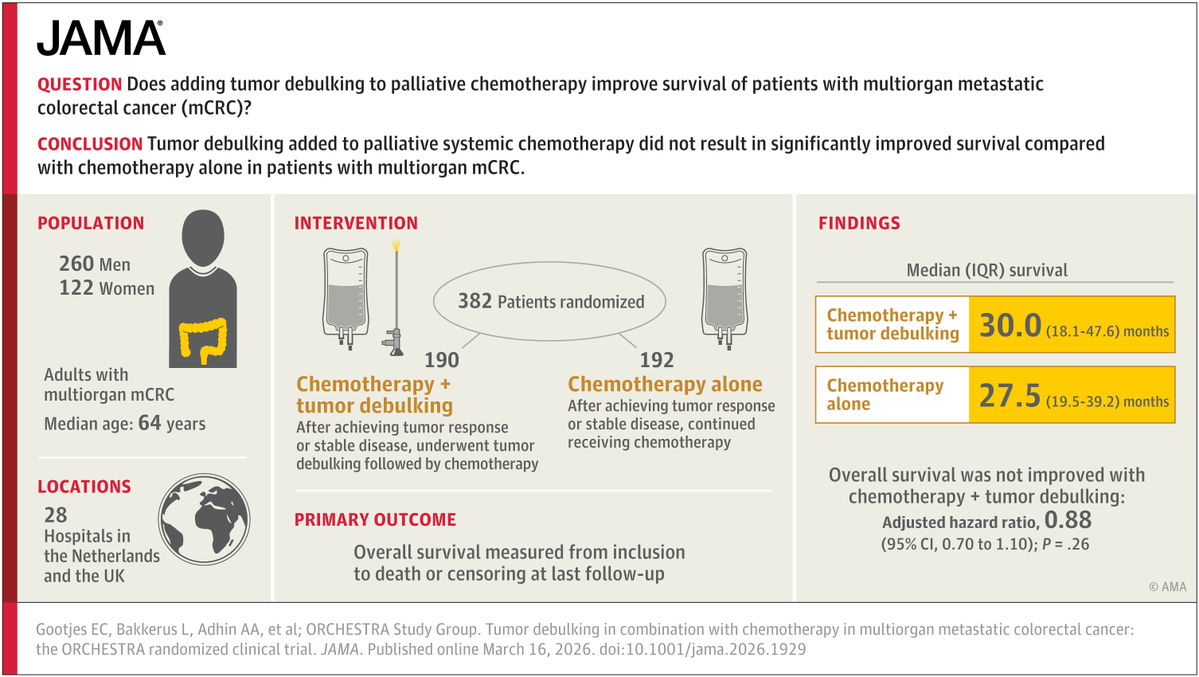
Tumor Debulking in Combination With Chemotherapy in Multiorgan Metastatic Colorectal Cancer: The ORCHESTRA Randomized Clinical Trial
@JAMAOnc
doi.org/10.1001/jama.2…
🧐even with modern chemotherapies, tumor debulking does not add anything....
@myESMO @ASCO
English
Jean Bustamante-Alvarez MD MS retweetledi

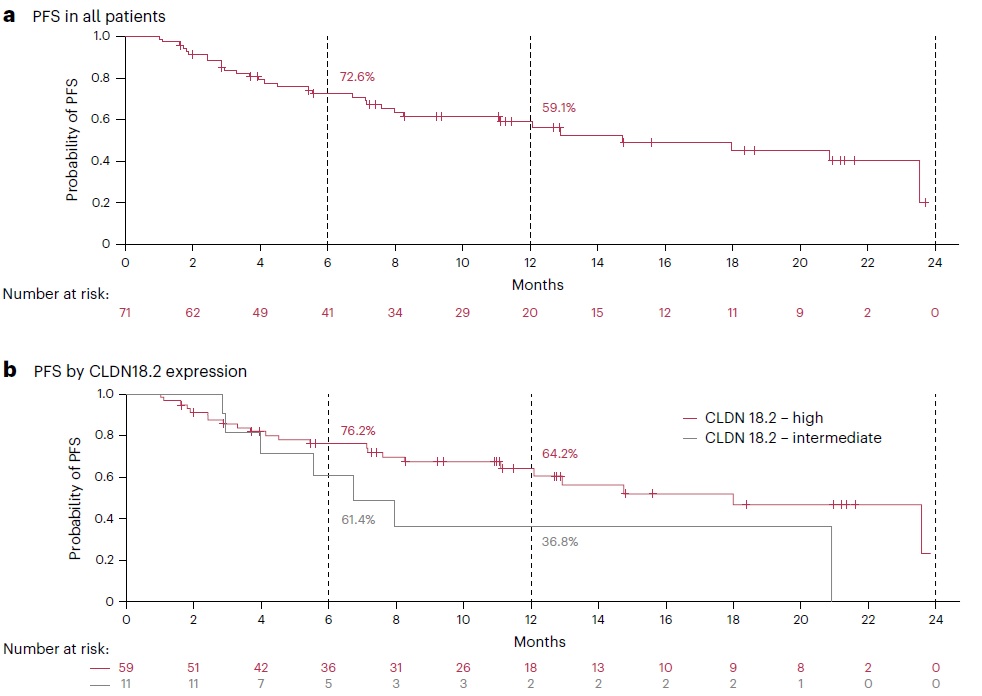
Delighted to share results of phase 2 ILUSTRO in @NatureMedicine @KlempnerSam @ASCOPost Zolbetuximab+FOLFOX+nivo showed encouraging activity in CLDN18.2+ gastric cancer with mPFS 14.8 months (18months in high CLDN). Supporting the ongoing phase 3 LUCERNA.
doi.org/10.1038/s41591…
English
Jean Bustamante-Alvarez MD MS retweetledi

Phase I ARTEMIS-001 trial of the B7-H3 ADC HS-20093 (GSK5764227) now @Cancer_Cell. In SCLC, RR 52%, DOR 7.1m with greater RR if topoisomerase I inhibitor naive vs treated (60% vs 17%), but no difference by platinum sensitivity. B7-H3 IHC not predictive.
cell.com/cancer-cell/fu…
English
Jean Bustamante-Alvarez MD MS retweetledi

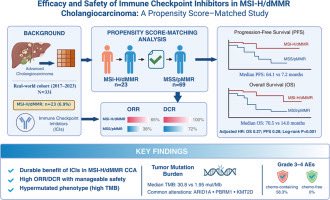
🧬 MSI-H/dMMR cholangiocarcinoma
📍 Real-world propensity-matched study (JHEP Reports)
👥 331 pts | MSI-H/dMMR: 6.9%
📊 ICIs-based therapy
• mPFS 64.1 vs 7.2 mo
• mOS 70.5 vs 14.0 mo (vs MSS)
🎯 MSI-H/dMMR emerges as a key predictive biomarker
🔗 doi.org/10.1016/j.jhep…
@GrupoTTD @OncoAlert
HT
Jean Bustamante-Alvarez MD MS retweetledi

Next-generation KRAS G12C inhibitor olomorasib shows promising pan-tumor activity in a first-in-human study.
ORR ~37% in non-CRC tumors with durable response.
Activity even observed after prior KRAS G12C inhibitors.
KRAS targeting keeps evolving.
nature.com/articles/s4146…


English
Jean Bustamante-Alvarez MD MS retweetledi

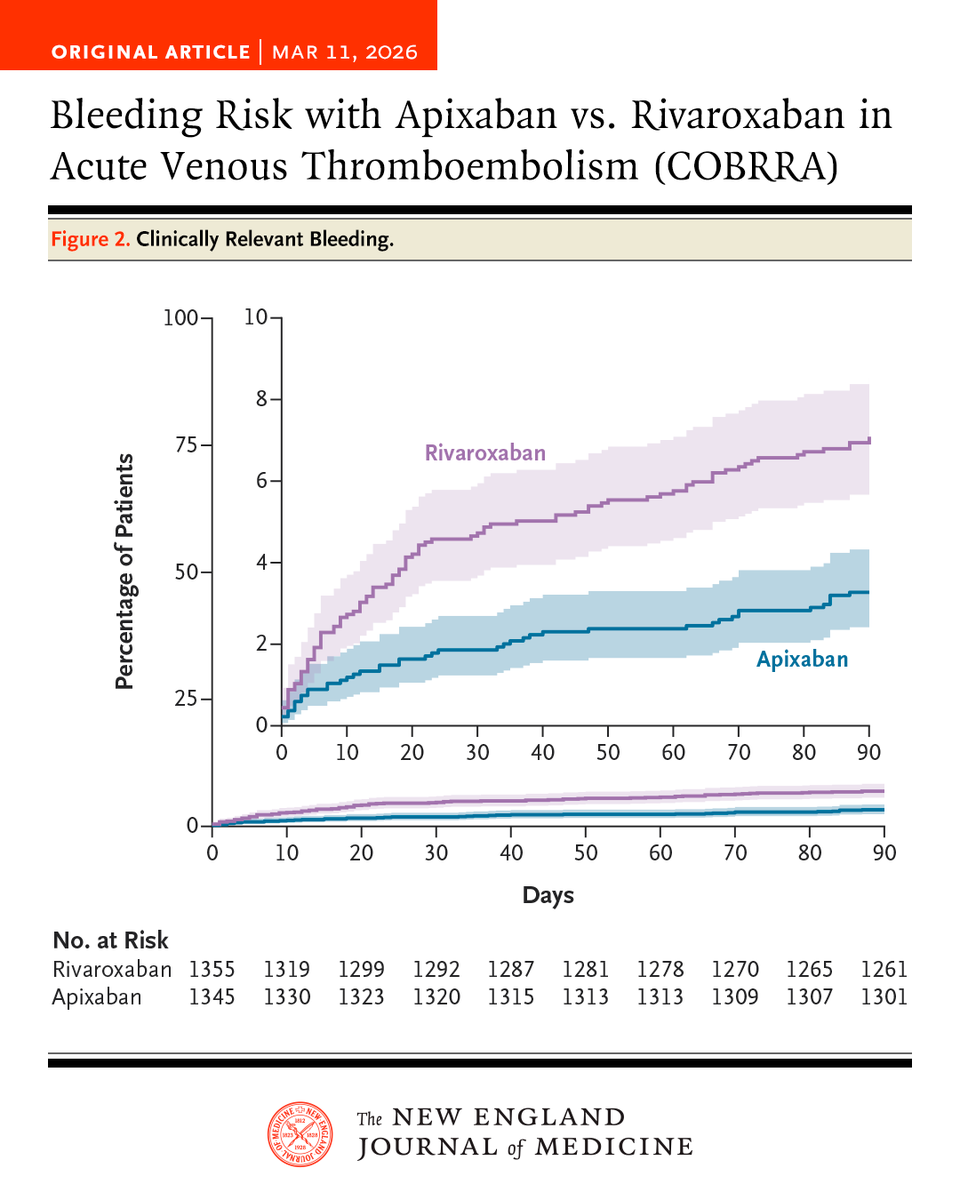
In an international, randomized trial involving patients with acute venous thromboembolism, the risk of clinically relevant bleeding was significantly lower with apixaban than with rivaroxaban during the 3-month treatment period.
Full COBRRA trial results: nejm.org/doi/full/10.10…
English
Jean Bustamante-Alvarez MD MS retweetledi
RECITE: In a phase 3 trial in patients with persistent chemotherapy-induced thrombocytopenia, 84% of those receiving romiplostim had no chemotherapy dose modifications, as compared with 36% of those receiving placebo (odds ratio, 10.16). Full trial results: nejm.org/doi/full/10.10…
Editorial: Thrombopoietin-Receptor Agonists in Chemotherapy-Induced Thrombocytopenia nejm.org/doi/full/10.10…
English
Jean Bustamante-Alvarez MD MS retweetledi

🎉Our latest research published in @CCR_AACR.
doi.org/10.1158/1078-0…
We provide the most comprehensive multiomic🧬 characterization to date of the B-cell 🫧 mediated immune response in resectable NSCLC 🫁 treated with perioperative chemoimmunotherapy (ChIO). @MARIANOPROVENCI

English
Jean Bustamante-Alvarez MD MS retweetledi
Jean Bustamante-Alvarez MD MS retweetledi
Have you ever wondered whether you need to hold systemic during RT due to concern for additive toxicity?
See this 10 min video.
Categorized by systemic type (cytoxic chemo, IO, TKI, BRAF, etc) & RT regimen (SBRT/conventional/palliative)
Slides🧵& full video below. 1/8
English
Jean Bustamante-Alvarez MD MS retweetledi

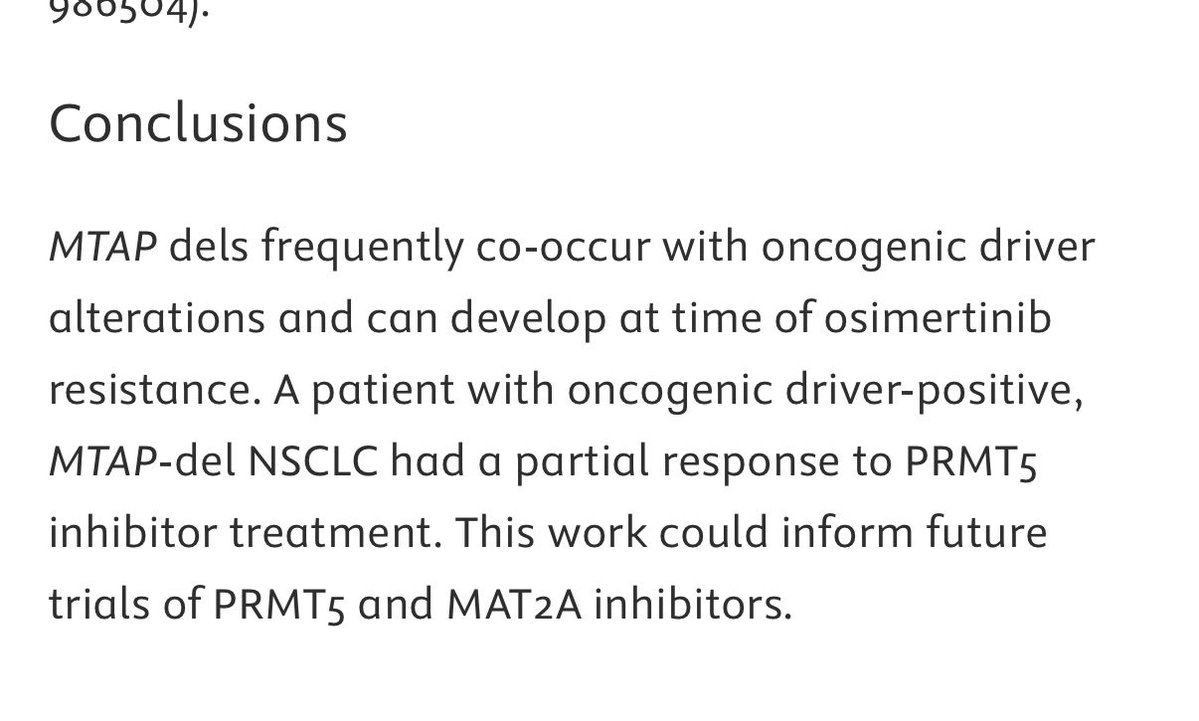
Clinical Significance of MTAPDeletions and Their Overlap With Concurrent Oncogenic Driver Alterations Including EGFR in NSCLC
jto.org/article/S1556-…
English
Jean Bustamante-Alvarez MD MS retweetledi


Jean Bustamante-Alvarez MD MS retweetledi

Radiotherapy Review in NEJM:
“Underuse and refusal of indicated radiotherapy have been shown to increase cancer-specific mortality and the risk of death in both curative and palliative settings”
nejm.org/doi/full/10.10…
English
Jean Bustamante-Alvarez MD MS retweetledi
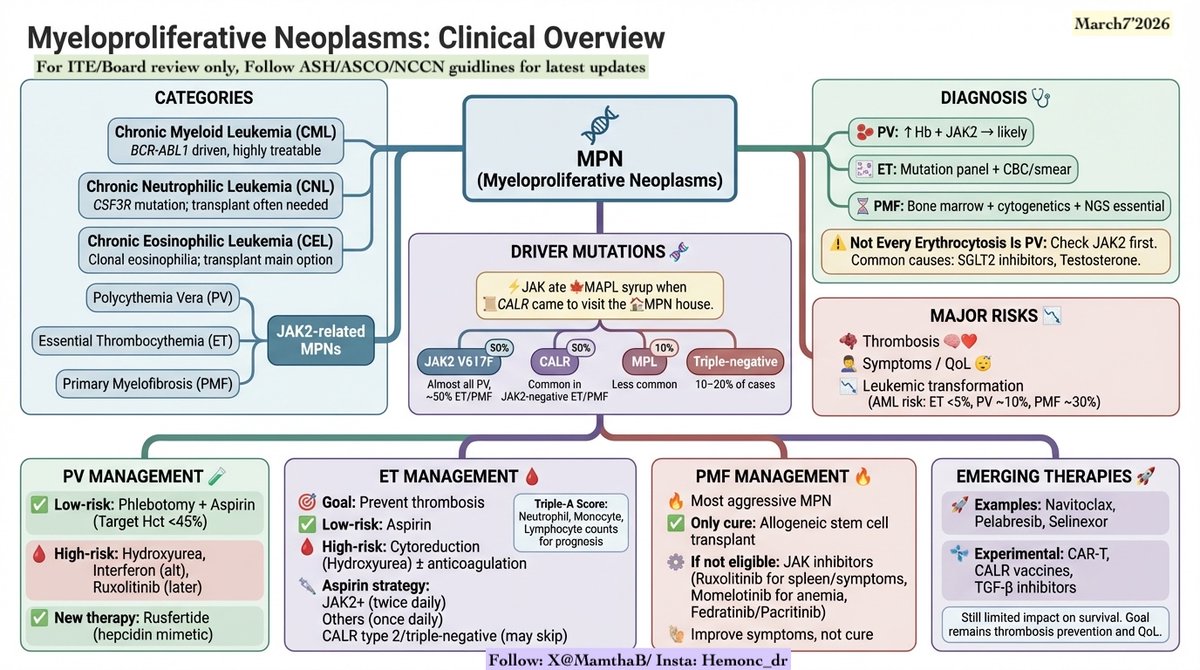
MPN (Myeloproliferative Neoplasms)
Board/ITE Key Clinical Pearls 🩸🧬
Mnemonic🙂
“⚡JAK ate 🍁MAPL syrup when 📜CALR came to visit the 🏠MPN house''
MPN Categories
🔹 Chronic Myeloid Leukemia – BCR-ABL1 driven, highly treatable
🔹 Chronic Neutrophilic Leukemia – CSF3R mutation; transplant often needed
🔹 Chronic Eosinophilic Leukemia – clonal eosinophilia; transplant main option
🔹 JAK2-related MPNs:
• Polycythemia Vera
• Essential Thrombocythemia
• Primary Myelofibrosis
Driver Mutations 🧬
⚡ JAK2 V617F – almost all PV, ~50% ET/PMF
⚡ CALR – common in JAK2-negative ET/PMF
⚡ MPL – less common
⚡ 10–20% triple-negative
Diagnosis 🩺
• PV: ↑Hb + JAK2 → diagnosis likely
• ET: mutation panel (JAK2/CALR/MPL) + CBC/smear
• PMF:bone marrow + cytogenetics + NGS essential
Not Every Erythrocytosis Is PV ⚠️
Common causes:
💊 SGLT2 inhibitors
💊 Testosterone
➡️ Check JAK2 first ➡️ Don’t stop beneficial meds automatically
Major Risks in MPNs
• Thrombosis
• Symptoms / QoL 😴
• Leukemic transformation
AML risk: • ET <5% • PV ~10% • PMF ~30%
ET Management 🩸 🎯: prevent thrombosis
PLT>450X109/L
🦶 Erythromelalgia, 🤕 Headache, 🩸 Clots
🔍 Diagnosis: BM Biopsy with predominent predominant
Risk factor: prior thrombosis
Platelet number is not a risk factor for thrombosis!!!
Treatment:
🟢 Low-risk (<60 no clot) → Aspirin
🔴 High-risk (>60 +/- clot) → Cyto reduction (Hydroxyurea) ± anticoagulation
Aspirin strategy: • JAK2+ (High risk of thrombosis) → twice daily • Others → once daily • CALR type 2 / triple-negative → may skip aspirin
The "Triple-A" Score: Modern prognosis in ET now uses Absolute Neutrophil, Monocyte, and Lymphocyte counts to identify patients who will live as long as the general population.
PV Management
🧪 Low-risk: 🩸 Phlebotomy + Aspirin 🎯 Hct <45% or Females <16, Males <16.5
High-risk:
💊 Hydroxyurea (Cytoreductive therapy-1L)
💊 Interferon (alternative)
💊 Ruxolitinib (2L- line-✅ Pruritis, 📉 Decreases EFS)
💊 Buslphan (Older patients )
New therapy:
💉 Ropeginterferon-alfa (FDA approval recently)
💉 Rusfertide – hepcidin mimetic (reduces phlebotomy)
Myelofibrosis 🔥 → Most aggressive MPN.
Night Sweats, 🌡️ Fever, 🦴 Bone Pain, Weight Loss, Organomegaly Hepatomegaly & Splenomegaly), Cytopenia, insomnia, fatigue, early satiety, abdominal pain
📊 IPSS Scoring System: Risk Groups
📉🧬Worsening prognosis: CALR+ (22.7%-17.7 yr)—>JAK2+ (65%-9.2yr) or MPL+ (4%-3.2yr)—> Triple Negative. (8.6%)
🚨High Molecular risk: 🧬IDH1/2, EZH2, ASXL1, SRSF2
Only cure: 🏥 Allogeneic stem cell transplant
If not eligible:
->Low risk/not symptomatic: observation
->Low risk/symptomatic: clinical trial/ruxolitinib/peginterferon /hydroxyuria
->High risk: transplant elgible-allo HSCT 💊 JAK inhibitors
1. Ruxolitinib – best tolerated and for spleen size and constitutional symptoms- Side effects-Zoster, TB activation, avoid interruptions causes SIRS so bridge with steroids
2. Momelotinib (MF+Anemia)(SE-Peripheral neuropathies) – helpful for anemia
3. Fedratinib-2L (SE-GI, WE (monitor thiamine)
4. Pacritinib (ACVR1- MF + platelets <50k or anemia)
->No constitutuation symptoms/splenomegaly
1. EPO>500mIU/ml→Luspatercept, danzol, iMids
2. EPO<500mIU/ML→ESA
➡️ Improve symptoms & spleen ❌ Do not cure disease
Emerging Therapies 🚀
• Navitoclax • Pelabresib • Selinexor
-CAR-T, CALR vaccines, TGF-β inhibitors- are in development
🧬 Clonal Eosinophilia
🧪 Key Molecular Screens
1. FIP1L1–PDGFRA: 🧬 (~10% of HES). Detect via FISH (look for CHIC2 deletion) or RNA-Seq.
2. PDGFRB: 🧬Often an MDS/MPN overlap.
3. FGFR1: 🧬🔥 (8p11 syndrome). Highly aggressive; often transforms to AML/Lymphoma.
4. JAK2 Rearrangements: 🧬 (Not V617F mutation!).
💊 Targeted Treatment Table
->FIP1L1–PDGFRA- Imatinib- Exquisitely sensitive (100mg dose)
->PDGFRB- Imatinib - High response rates 👍
->FGFR1- Pemigatinib -Requires Chemo + Transplant ->JAK2 Rearr-Ruxolitinib -Specific for rearrangements- CEL-NOSCytoreduction 📉Diagnosis of exclusion 🔍
Chronic Neutrophilic Leukemia (CNL) 🩸
Hallmark: CSF3R mutation (G-CSF receptor). 🧬🔗
Presentation: Neutrophils/Bands >80% + Splenomegaly
Treatment: Ruxolitinib (Symptom relief) ➡️ SCT 🏥 (Curative).
Systemic Mastocytosis (SM) 🐝
Hallmark: KIT D816V mutation. 🧬
Physical Exam: Darier Sign (rubbing skin causes hives) 🤏+ Urticaria Pigmentosa.
Markers: Tryptase 📈, CD25, and CD117 (KIT). 🧪
Treatment: Avapritinib or Midostaurin 🎯.
#Hematology #Oncology #MedEd #HemOnc #FOAMed #MPN #BoardReview #MedStudentTwitter #InternalMedicine #Pathology #MPN @ASH_hematology @MPNVoice @ASCOPost @IMG_Oncologists @OncoAlert @oncodaily @realbowtiedoc @VJHemOnc @JCO_ASCO
@LeukemiaJnl #HemOnc #MedTwitter #FOAMed
@HemOncFellows
English
Jean Bustamante-Alvarez MD MS retweetledi

Jean Bustamante-Alvarez MD MS retweetledi
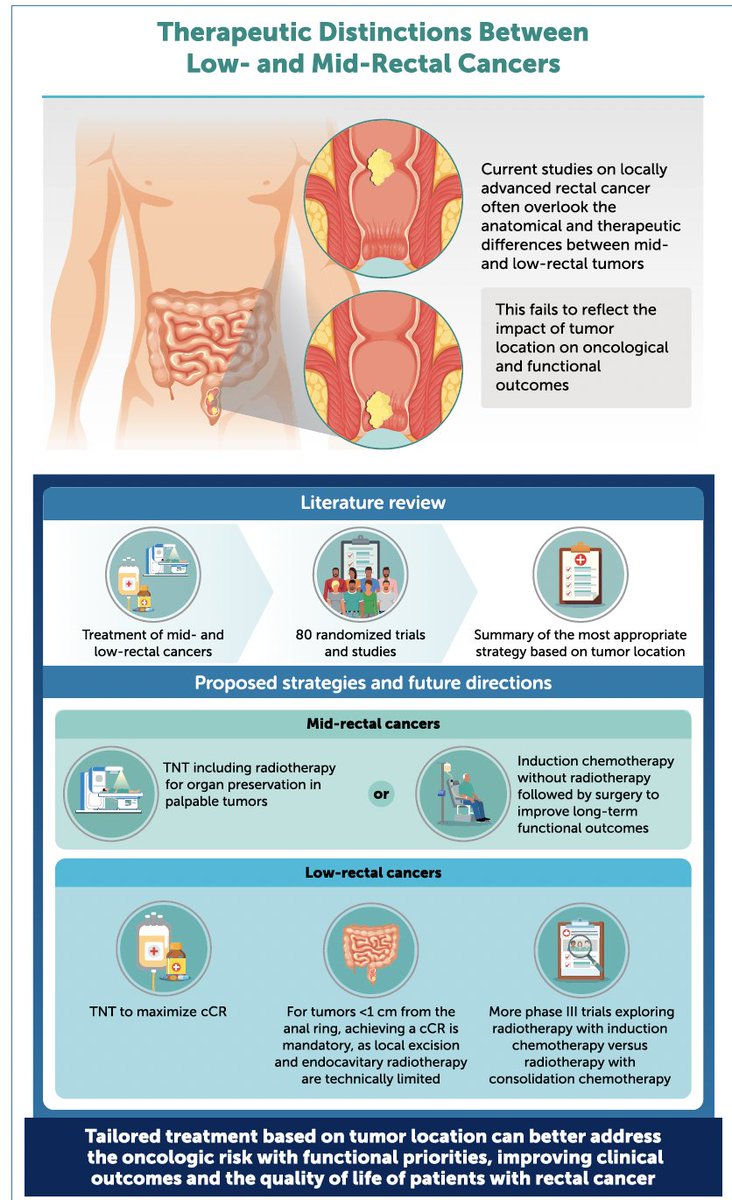
Disruptive Analysis of Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer: Clinical and Therapeutic Distinctions Between Lowand Mid-Rectal Cancers
@JCO_ASCO
doi.org/10.1200/JCO-25…
👏excellent review
👉Adopting a location-specific, patient-centered approach is key
@myESMO @ASCO
English