Sabitlenmiş Tweet

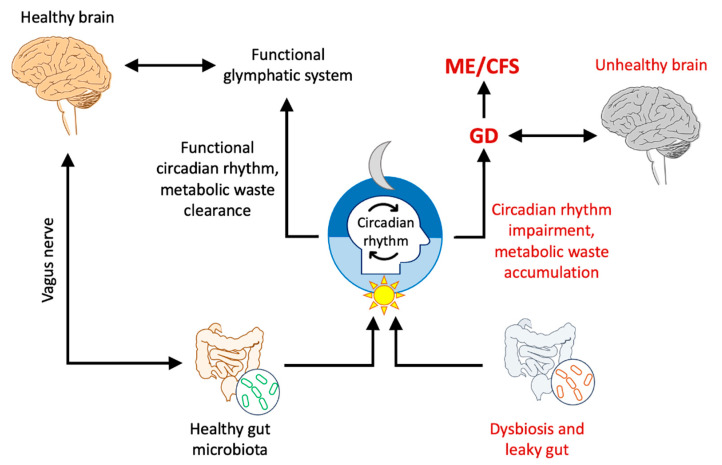
@StanfordMed researchers have shown Glymphatic System Dysregulation as a Key Contributor to Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. The glymphatic system is the brain's drainage system of toxins. Lymphatics carry these and when blocked cause disease. (paper link below)
English