Fathimath Naseer RD retweetledi

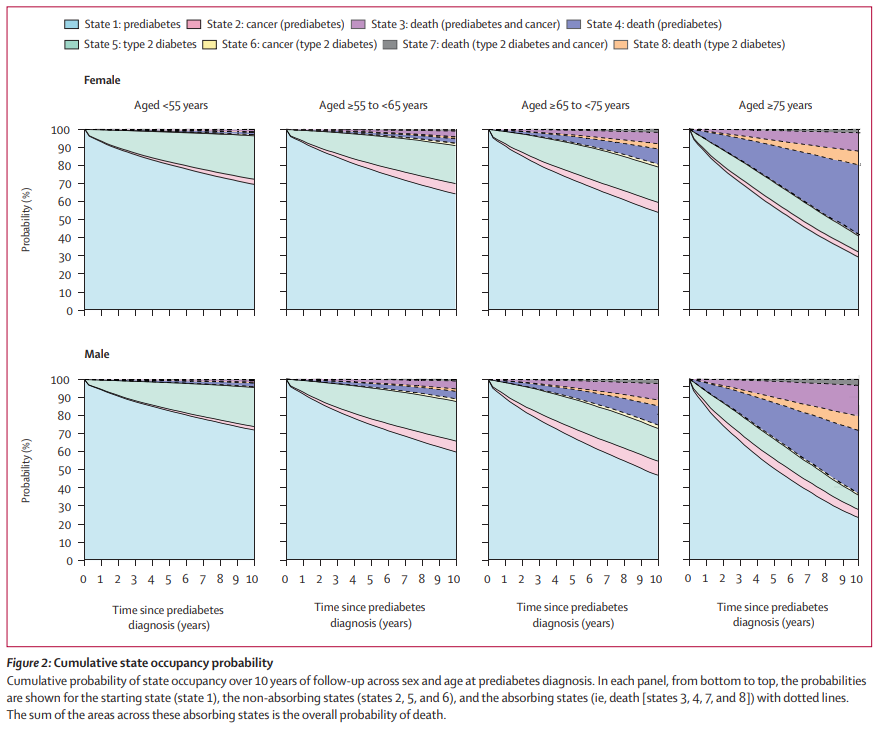
NEW: Trajectories of type 2 diabetes and cancer in 330 000 individuals with prediabetes: 20-year observational study in England
This study finds similar #cancer incidence rates following #prediabetes and type 2 #diabetes
thelancet.com/journals/landi…
English