
🩺 Pancreatic reconstruction after PD: Blumgart anastomosis does not reduce clinically relevant POPF compared with invaginating pancreatogastrostomy. @AnnalsofSurgery
🧪 Study overview
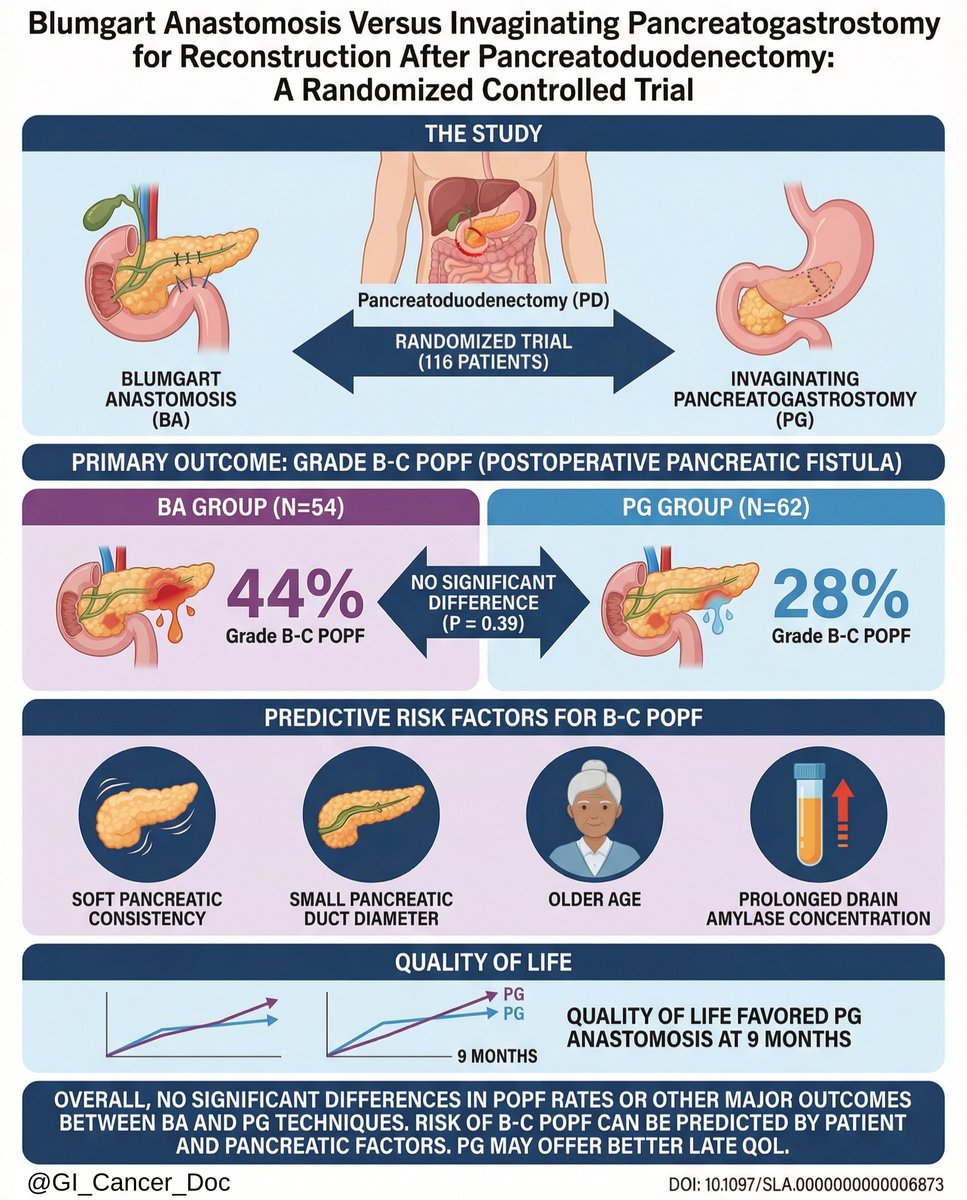
Randomized controlled trial comparing Blumgart anastomosis (BA) vs pancreatogastrostomy (PG) after pancreatoduodenectomy
Primary endpoint: postoperative pancreatic fistula (POPF), including clinically relevant grades
📊 Key findings
• Overall POPF rates were not significantly different between BA and PG
• Clinically relevant POPF occurred at comparable rates in both groups
• Severe complications and mortality were similar between techniques
• Pancreatic texture, duct diameter, and patient factors influenced POPF independent of reconstruction method
⚠️ Limitations noted
• Anastomotic technique alone did not overcome gland- and patient-related risk factors
💡 Clinical takeaway
Choice between BA and PG should be individualized, with greater emphasis on pancreatic risk profile and surgeon expertise than on anastomotic technique.
🔗 Source:
pubmed.ncbi.nlm.nih.gov/40747945
#AnnalsOfSurgery #Pancreatoduodenectomy #PancreaticSurgery #PostoperativePancreaticFistula #RandomizedControlledTrial #SurgicalReconstruction
English